

Impact of prostate biopsy technique on outcomes of the precision prostatectomy procedure
- PMID: 35892060
- PMCID: PMC9260793
- DOI: 10.1136/bmjsit-2021-000122
Impact of prostate biopsy technique on outcomes of the precision prostatectomy procedure
Abstract
Objective: To assess the impact of iterative changes in preoperative and postoperative biopsy techniques on the outcomes of men undergoing the precision prostatectomy procedure. Precision prostatectomy is a novel surgical treatment for prostate cancer that aims to maximally preserve erectogenic nerves via partial preservation of the prostate capsule.
Design: Retrospective.
Setting: Single tertiary care center.
Participants: This study included 120 patients who consented to undergo prostate cancer treatment with the precision prostatectomy procedure. Patients were originally enrolled in one of two separate prospective protocols studying precision prostatectomy.
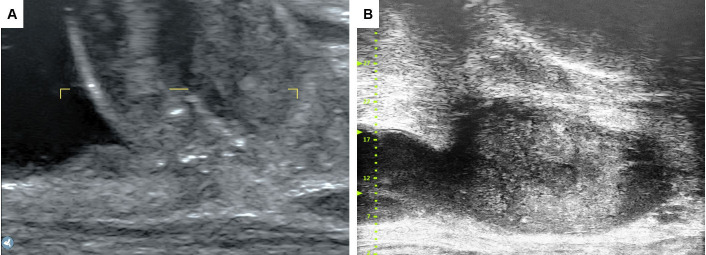
Interventions: Preoperatively, 60 patients were screened with transrectal (TR) biopsy and 60 were screened by transperineal (TP) biopsy. Ultimately, 117 patients underwent precision prostatectomy. Of the 43 postoperative biopsies, 19 were TR; 17 were TP with ultrasound; and 7 were TP with microultrasound (mUS).
Main outcome measures: Preoperatively, we evaluated whether the transition to TP biopsy was associated with differences in postoperative treatment failure defined as a neoplasm-positive postoperative biopsy. Postoperative biopsies were compared with respect to their ability to sample the remnant tissue, specifically percentage of cores positive for prostate tissue.
Results: Preoperatively, 9/60 (15%) positive postoperative biopsies occurred in the TR group and 6/60 (10%) in the TP group; Kaplan-Meier survival estimates did not differ between groups (p=0.69 by log rank). Postoperatively, the numbers of cores positive for prostate tissue were 99/160 (62%), 63/107 (59%), and 36/39 (92%) in the TR biopsy, TP with ultrasound, and TP with mUS groups, respectively; this difference was statistically significant versus the rate in the TR and standard TP groups (p=0.0003 and 0.0002).
Conclusion: We found no significant improvement in patient screening, preoperatively-though limited by small sample size and relatively short follow-up. The incorporation of high-frequency mUS for postoperative biopsies improved the ability to sample the remnant tissue with a higher efficiency.
Keywords: Robotic Surgical Procedures.
© Author(s) (or their employer(s)) 2022. Re-use permitted under CC BY-NC. No commercial re-use. See rights and permissions. Published by BMJ.
Conflict of interest statement
Competing interests: None declared.
Figures


References
LinkOut - more resources
Full Text Sources