

DNA methylation profiling improves routine diagnosis of paediatric central nervous system tumours: A prospective population-based study
- PMID: 35892159
- PMCID: PMC9543790
- DOI: 10.1111/nan.12838
DNA methylation profiling improves routine diagnosis of paediatric central nervous system tumours: A prospective population-based study
Abstract
Aims: Paediatric brain tumours are rare, and establishing a precise diagnosis can be challenging. Analysis of DNA methylation profiles has been shown to be a reliable method to classify central nervous system (CNS) tumours with high accuracy. We aimed to prospectively analyse CNS tumours diagnosed in Sweden, to assess the clinical impact of adding DNA methylation-based classification to standard paediatric brain tumour diagnostics in an unselected cohort.
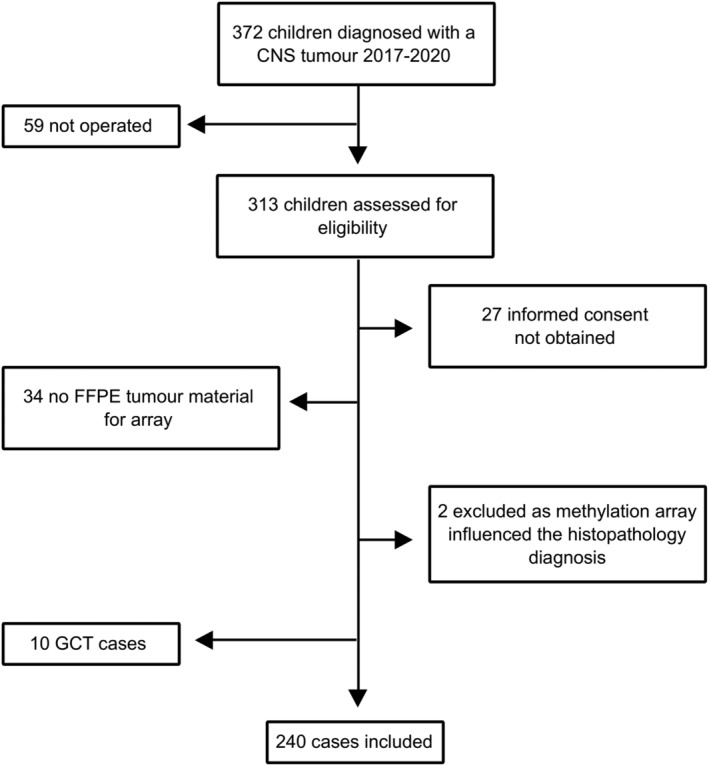
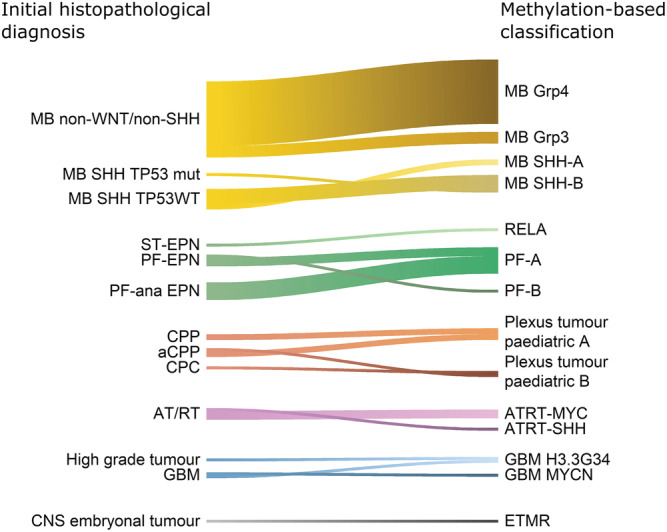
Methods: All CNS tumours diagnosed in children (0-18 years) during 2017-2020 were eligible for inclusion provided sufficient tumour material was available. Tumours were analysed using genome-wide DNA methylation profiling and classified by the MNP brain tumour classifier. The initial histopathological diagnosis was compared with the DNA methylation-based classification. For incongruent results, a blinded re-evaluation was performed by an experienced neuropathologist.
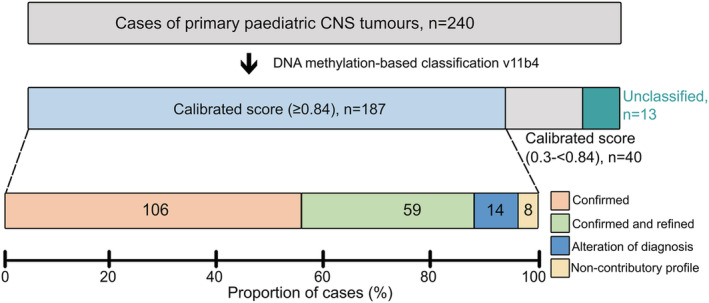
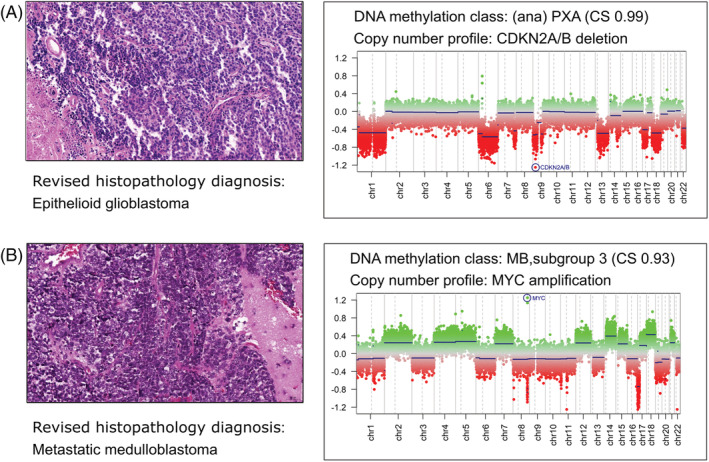
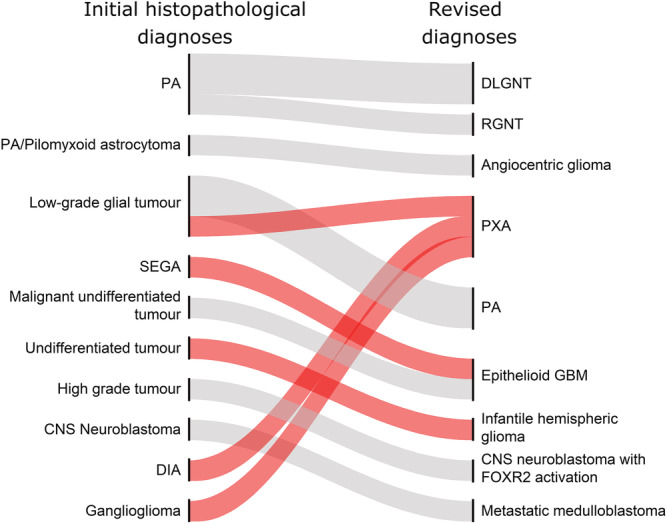
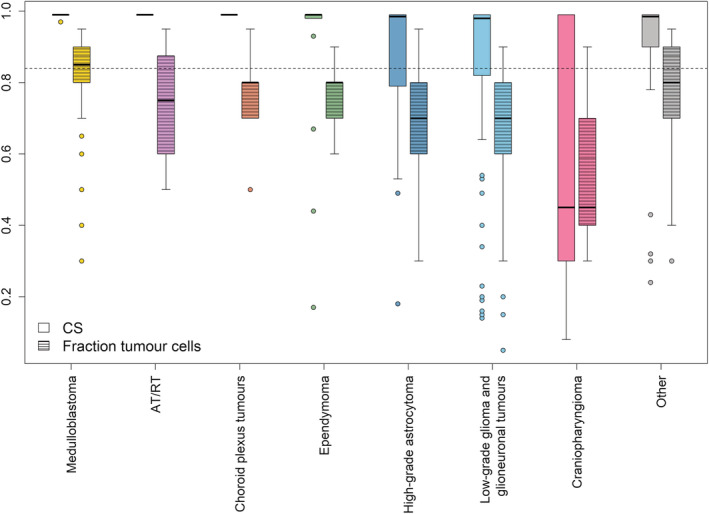
Results: Two hundred forty tumours with a histopathology-based diagnosis were profiled. A high-confidence methylation score of 0.84 or more was reached in 78% of the cases. In 69%, the histopathological diagnosis was confirmed, and for some of these also refined, 6% were incongruent, and the re-evaluation favoured the methylation-based classification. In the remaining 3% of cases, the methylation class was non-contributory. The change in diagnosis would have had a direct impact on the clinical management in 5% of all patients.
Conclusions: Integrating DNA methylation-based tumour classification into routine clinical analysis improves diagnostics and provides molecular information that is important for treatment decisions. The results from methylation profiling should be interpreted in the context of clinical and histopathological information.
Keywords: DNA methylation profiling; diagnostics; molecular classification; paediatric brain tumours.
© 2022 The Authors. Neuropathology and Applied Neurobiology published by John Wiley & Sons Ltd on behalf of British Neuropathological Society.
Conflict of interest statement
SMP declare patent PCT/EP2016/055337 DNA‐methylation‐based method for classifying tumour species. All other authors have no conflicts of interest to report.
Figures
References
-
- Louis DN, Ohgaki H, Wiestler OD, Cavenee WK. WHO Classification of Tumours of the Central Nervous System. 4thed. International Agency for Research on Cancer (Lyon); 2016.
-
- Gustafsson G, Kogner P, Heyman M. Childhood cancer incidence and survival in Sweden 1984‐2010, Report 2013:2013.
