

Is There a Place for Adjuvant Chemotherapy in the Treatment of Locally Advanced Cervical Cancer?
- PMID: 35892984
- PMCID: PMC9332289
- DOI: 10.3390/curroncol29080415
Is There a Place for Adjuvant Chemotherapy in the Treatment of Locally Advanced Cervical Cancer?
Abstract
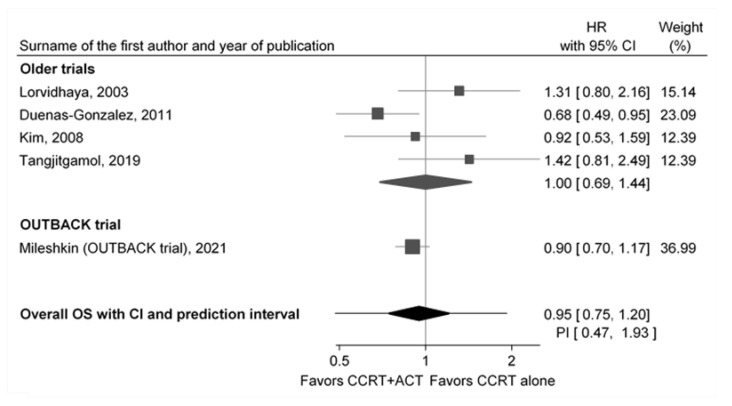
Findings on the efficacy of adjuvant chemotherapy (ACT) of locally advanced cervical cancer (LACC) after the concurrent chemoradiation (CCRT) therapy were inconsistent, and the OUTBACK trial was expected to shed some light regarding the topic. Its results on ACT in LACC were negative, with the conclusion of not to use it. The objective of this review was to present the inconsistencies of previous studies, along with the OUTBACK trial in more detail, and to rethink whether its results provide an unambiguous and definite answer to the optimal position of ACT in the treatment of LACC. To critically appraise the OUTBACK trial and understand the consequences of its results, we used only randomized controlled studies (RCTs) on ACT in LACC that have been included in high-quality systematic reviews and meta-analyses. We calculated the pooled prediction intervals using a random effects meta-analysis of all published randomized studies including the OUTBACK trial. After combining the OUTBACK trial with the results of four previous randomized trials, the pooled hazard ratio for overall survival benefit of CCRT + ACT was 0.95 (95% CI 0.75; 1.20). The pooled hazard ratio of the four previous trials was 1.00 (95% CI 0.69; 1.44). The OUTBACK trial improved the precision of the pooled estimate, but the clinical heterogeneity and the consequent prediction intervals are still very wide, and with 95% reliability, we can expect that if the new study, using a similar approach to the ACT, on a randomly selected patient population from the presented five trials is conducted, its hazard ratio for overall survival after ACT would be between 0.47 and 1.93. In conclusion, there is an absolute need for further research in order to optimally define the position of ACT in the treatment of LACC.
Keywords: adjuvant chemotherapy; concurrent chemoradiation; locally advanced cervical cancer; uterine cervical neoplasms.
Conflict of interest statement
Dora Čerina, Tihana Boraska Jelavić, Matea Buljubašić Franić, Krešimir Tomić, Žarko Bajić, and Eduard Vrdoljak declare that they have no competing interests.
Figures
References
-
- Tan L.-T., Pötter R., Sturdza A., Fokdal L., Haie-Meder C., Schmid M., Gregory D., Petric P., Jürgenliemk-Schulz I., Gillham C., et al. Change in Patterns of Failure After Image-Guided Brachytherapy for Cervical Cancer: Analysis from the RetroEMBRACE Study. Int. J. Radiat. Oncol. 2019;104:895–902. doi: 10.1016/j.ijrobp.2019.03.038. - DOI - PubMed
-
- Keys H.M., Bundy B.N., Stehman F.B., Muderspach L.I., Chafe W.E., Suggs C.L., Walker J.L., Gersell D. Cisplatin, Radiation, and Adjuvant Hysterectomy Compared with Radiation and Adjuvant Hysterectomy for Bulky Stage IB Cervical Carcinoma. N. Engl. J. Med. 1999;340:1154–1161. doi: 10.1056/NEJM199904153401503. - DOI - PubMed
-
- Morris M., Eifel P.J., Lu J., Grigsby P.W., Levenback C., Stevens R.E., Rotman M., Gershenson D.M., Mutch D.G. Pelvic Radiation with Concurrent Chemotherapy Compared with Pelvic and Para-Aortic Radiation for High-Risk Cervical Cancer. N. Engl. J. Med. 1999;340:1137–1143. doi: 10.1056/NEJM199904153401501. - DOI - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
