

High Neutrophil-Lymphocyte Ratio and Low Lymphocyte-Monocyte Ratio Combination after Thrombolysis Is a Potential Predictor of Poor Functional Outcome of Acute Ischemic Stroke
- PMID: 35893315
- PMCID: PMC9332832
- DOI: 10.3390/jpm12081221
High Neutrophil-Lymphocyte Ratio and Low Lymphocyte-Monocyte Ratio Combination after Thrombolysis Is a Potential Predictor of Poor Functional Outcome of Acute Ischemic Stroke
Abstract
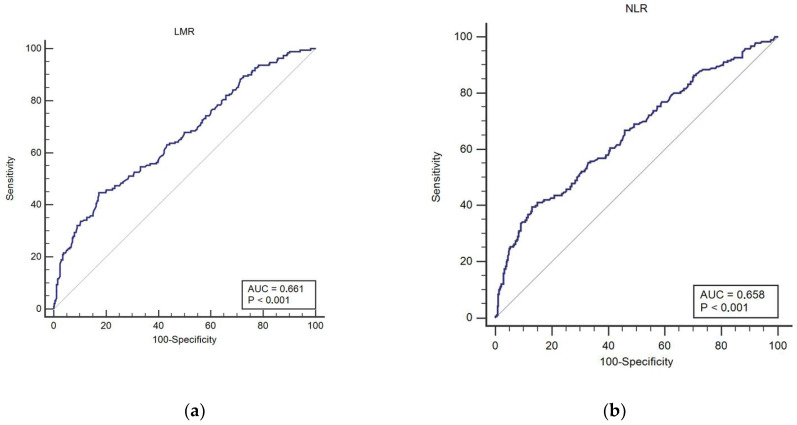
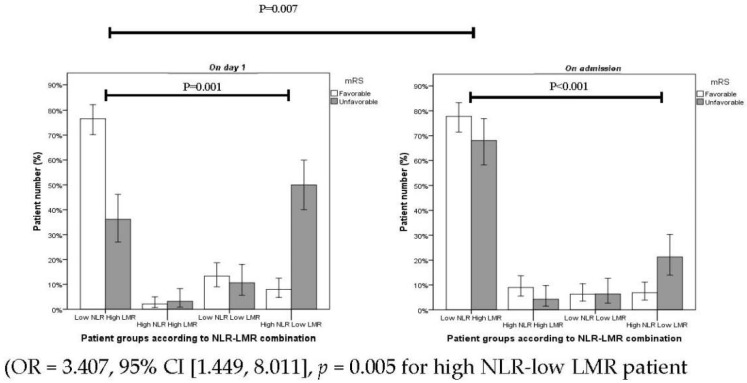
(1) Background: Ischemic stroke is one of the leading causes of death and disability. An inflammatory response is observed in multiple stages of cerebral ischemia, particularly in the acute phase. Recent publications revealed that the neutrophil−lymphocyte ratio (NLR) and lymphocyte−monocyte ratio (LMR) may be used to predict long-term prognosis in acute ischemic stroke (AIS) after thrombolysis. To test whether there is a relationship between the combination of these parameters and long-term prognosis, we analyzed the NLR−LMR combination in AIS patients treated with intravenous recombinant tissue plasminogen activator (rtPA); (2) Methods: The study included 285 adults with a diagnosis of AIS and rtPA treatment within a 4.5 h time window. Blood samples were obtained at admission and 24 h after thrombolysis to calculate pre- and post-thrombolysis NLR and LMR. Clinical data, including NIHSS was registered on admission and day 1. The long-term outcome was defined 90 days post-event by the modified Rankin Scale (mRS). Therapy-associated intracranial hemorrhage (ICH) was classified according to ECASS II. Receiver operating characteristic curve (ROC) analysis was performed to determine optimal cutoffs of NLR and LMR as predictors of therapy outcomes; (3) Results: Patients were stratified by cutoffs of 5.73 for NLR and 2.08 for LMR. The multivariate logistic regression model, including all possible confounders, displayed no significant association between NLR or LMR with 3-months functional prognosis. The combination of high NLR−low LMR vs. low NRL−high LMR as obtained 24 h after thrombolysis was found to be an independent predictor of poor 3-months functional outcome (mRS ≥ 2; OR 3.407, 95% CI 1.449 to 8.011, p = 0.005). The proportion of patients between low NLR−high LMR and high NLR−low LMR groups from admission to day 1 showed no significant change in the good outcome group. On the other hand, in the poor outcome group (mRS ≥ 2), low NLR−high LMR and high NLR−low LMR groups displayed a significant shift in patient proportions from 67% and 21% at admission (p = 0.001) to 36% and 49% at 24 h after thrombolysis (p < 0.001), respectively; (4) Conclusions: Our study demonstrated for the first time that a high NLR−low LMR combination as observed at 24 h after thrombolysis can serve as an independent predictor of 3-months poor outcome in AIS patients. This simple and readily available data may help clinicians to improve the prognostic estimation of patients and may provide guidance in selecting patients for personalized and intensified care post-thrombolysis.
Keywords: ischemic stroke; lymphocyte-monocyte ratio; neutrophil-lymphocyte ratio; thrombolysis.
Conflict of interest statement
The authors declare no conflict of interest.
Figures
References
-
- Feigin V.L., Stark B.A., Johnson C.O., Roth G.A., Bisignano C., Abady G.G., Abbasifard M., Abbasi-Kangevari M., Abd-Allah F., Abedi V., et al. Global, regional, and national burden of stroke, 1990–2016: A systematic analysis for the Global Burden of Disease Study 2016. Lancet Neurol. 2019;18:439–458. doi: 10.1016/S1474-4422(18)30499-X. - DOI - PMC - PubMed
Grants and funding
LinkOut - more resources
Full Text Sources
