

Tuberculosis of the Heart: A Diagnostic Challenge
- PMID: 35894002
- PMCID: PMC9326682
- DOI: 10.3390/tomography8040137
Tuberculosis of the Heart: A Diagnostic Challenge
Abstract
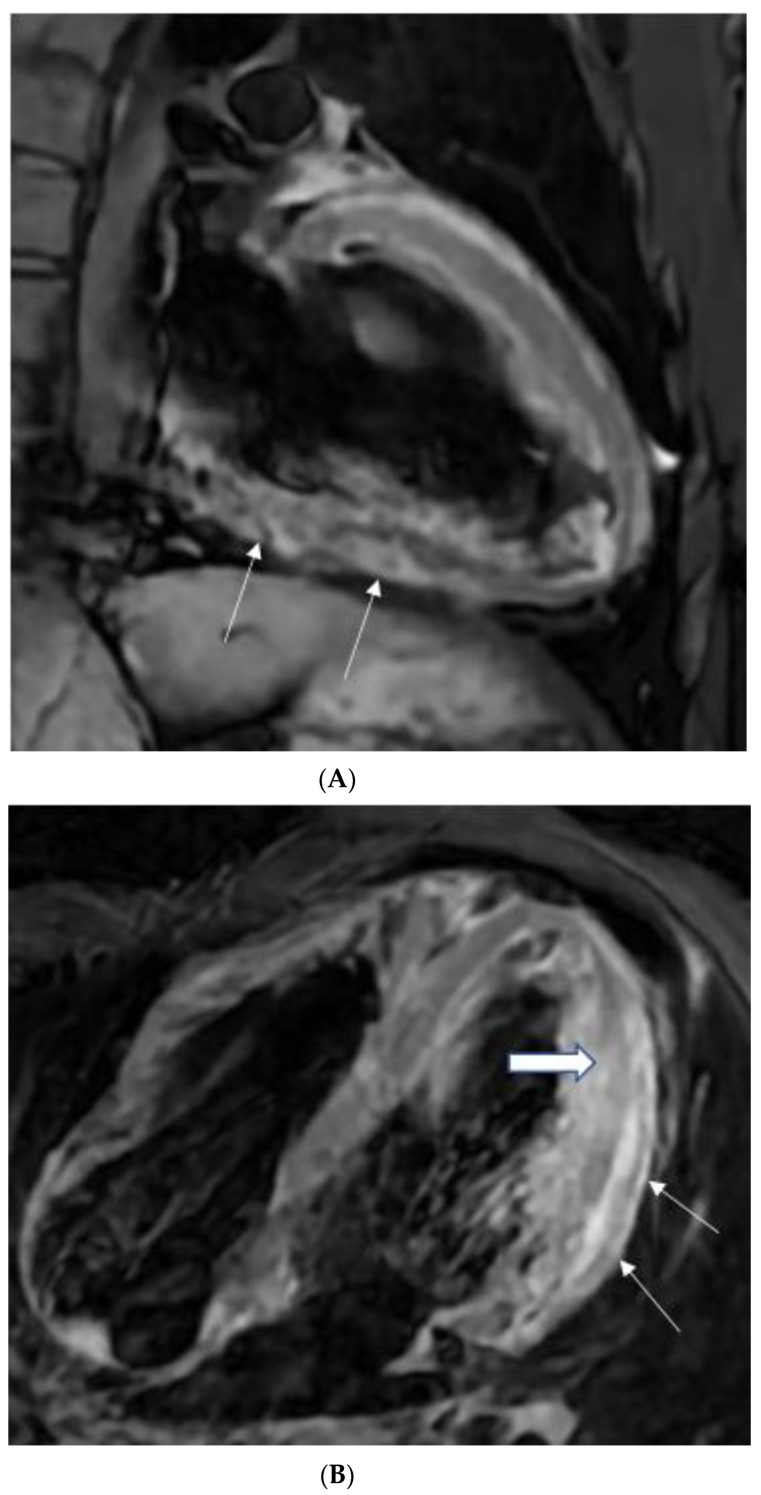
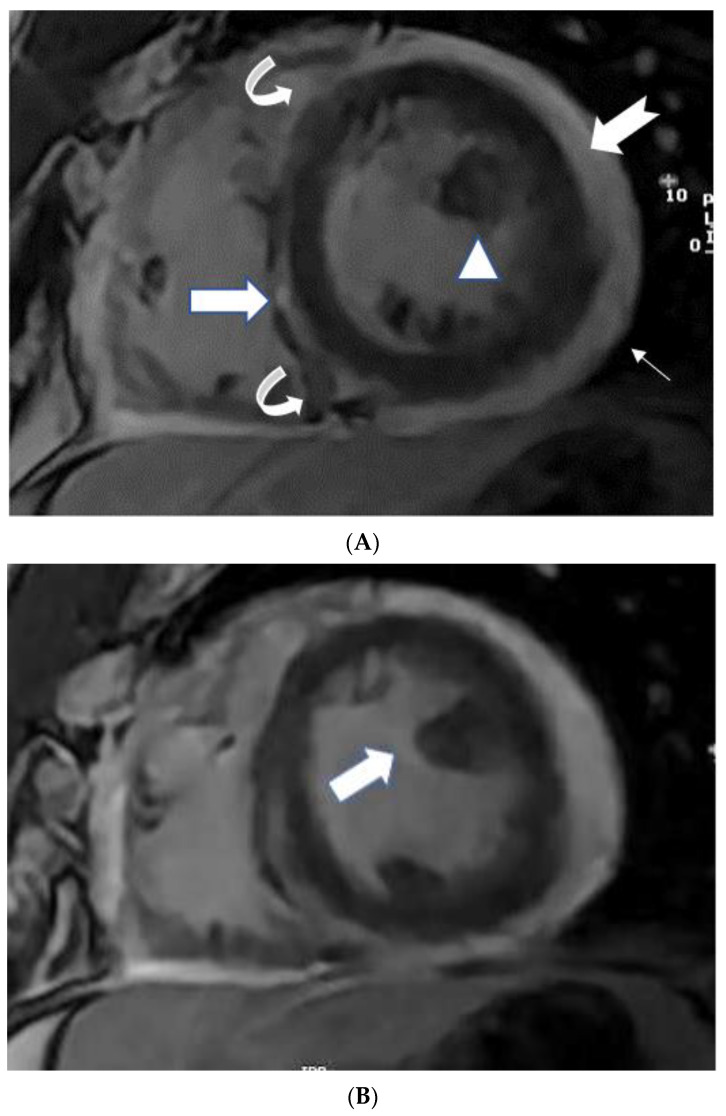
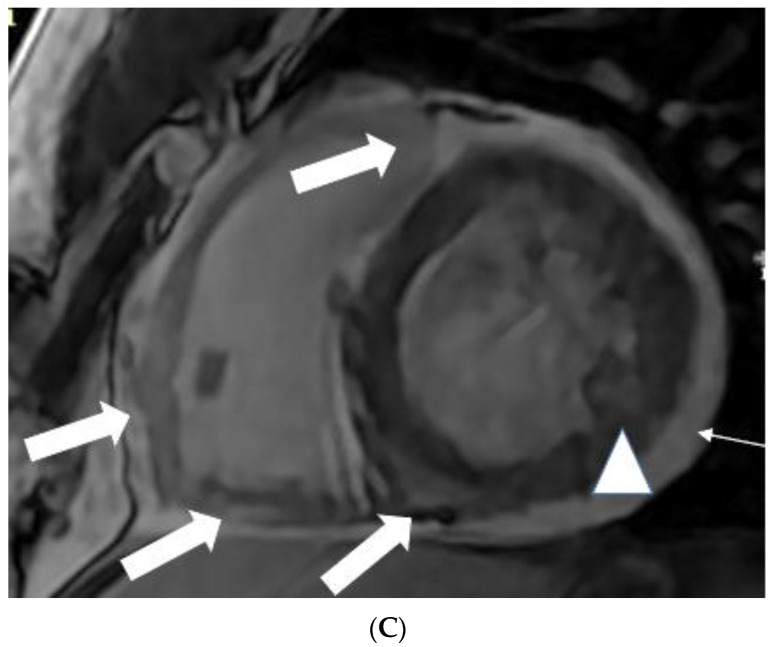
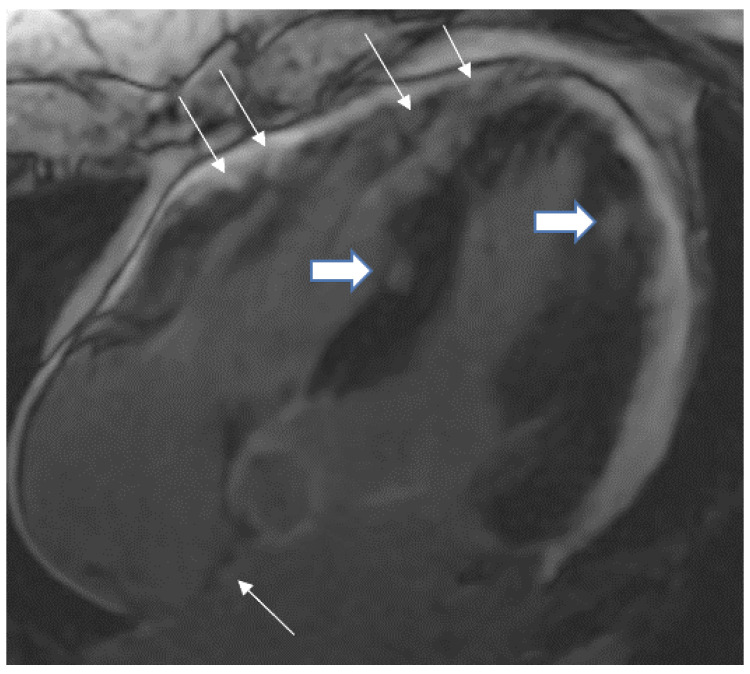
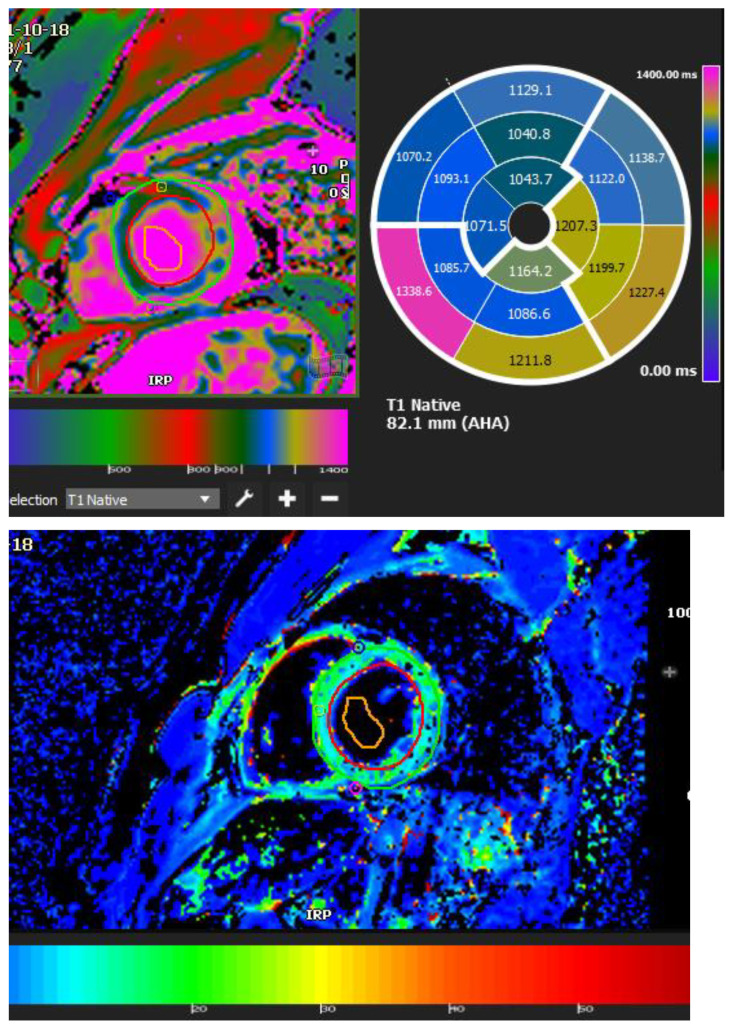
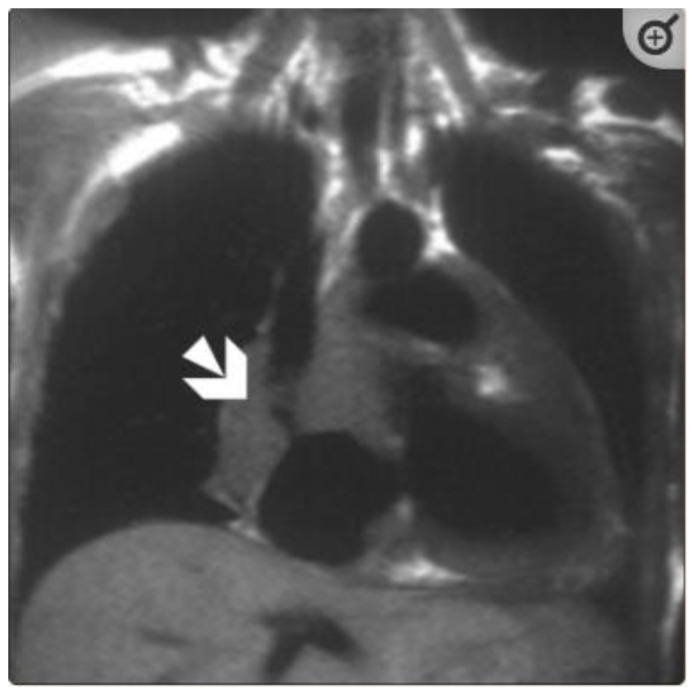
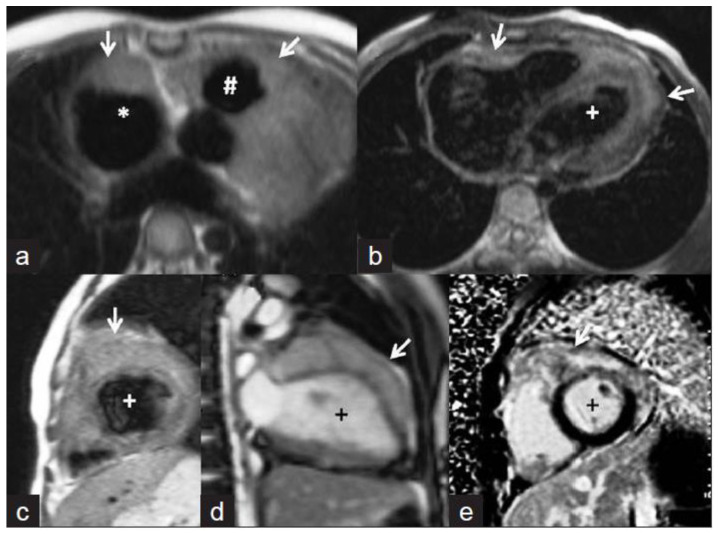
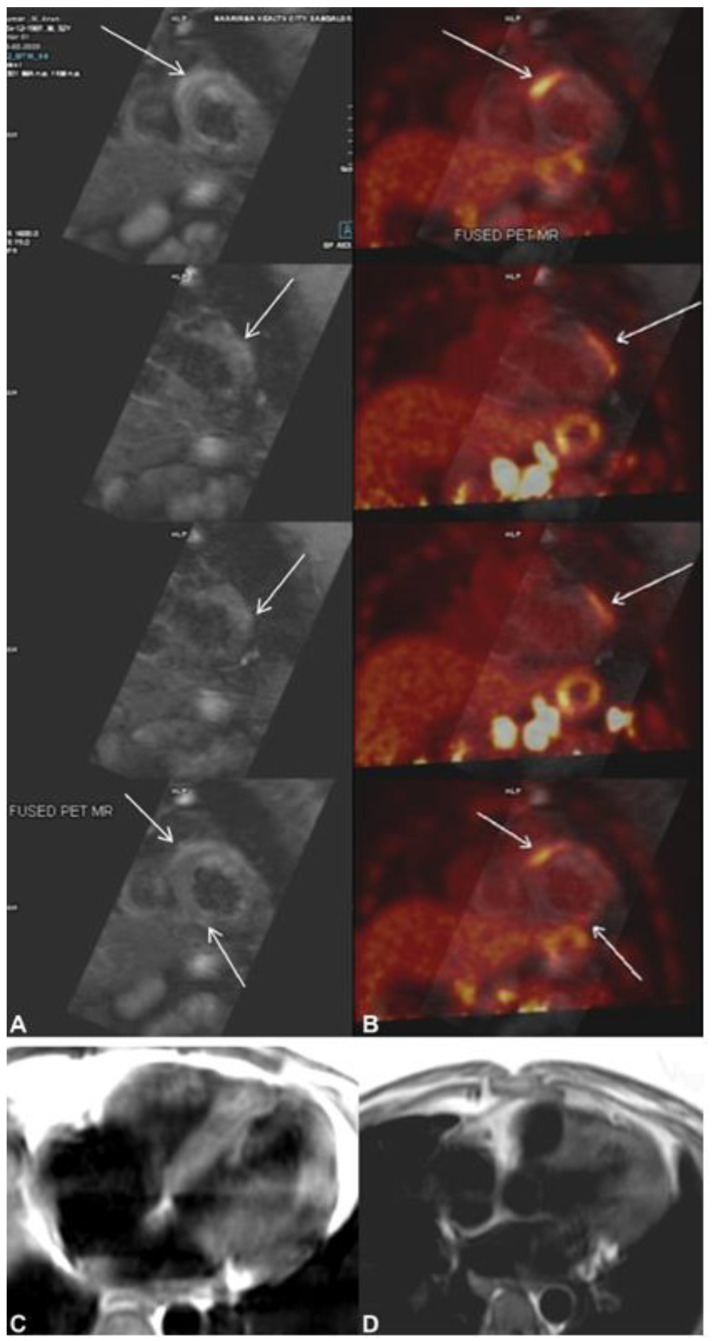
Tuberculosis of the heart is relatively rare and presents a significant diagnostic difficulty for physicians. It is the leading cause of death from infectious illness. It is one of the top 10 leading causes of death worldwide, with a disproportionate impact in low- and middle-income nations. The radiologist plays a pivotal role as CMR is a non-invasive radiological method that can aid in identifying potential overlap and differential diagnosis between tuberculosis, mass lesions, pericarditis, and myocarditis. Regardless of similarities or overlap in observations, the combination of clinical and certain particular radiological features, which are also detected by comparison to earlier and follow-up CMR scans, may aid in the differential diagnosis. CMR offers a significant advantage over echocardiography for detecting, characterizing, and assessing cardiovascular abnormalities. In conjunction with clinical presentation, knowledge of LGE, feature tracking, and parametric imaging in CMR may help in the early detection of tuberculous myopericarditis and serve as a surrogate for endomyocardial biopsy resulting in a quicker diagnosis and therapy. This article aims to explain the current state of cardiac tuberculosis, the diagnostic utility of CMR in tuberculosis (TB) patients, and offer an overview of the various imaging and laboratory procedures used to detect cardiac tuberculosis.
Keywords: irregular thickening of pericardium; magnetic resonance imaging; transmural mesocardial and epicardial fat late enhancement; tuberculous myopericarditis.
Conflict of interest statement
The authors declare no conflict of interest.
Figures
References
-
- Horn H., Saphir O. The Involvement of the Myocardium in Tuberculosis, A Review of the Literature and Report of 3 Cases. Am. Rev. Tuberc. 1935;32:492–506.
-
- Njovane X. Intramyocardial tuberculosis: A rare underdiagnosed entity. SAMJ S. Afr. Med. J. 2009;99:152–153. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
