

A Novel Method for Lung Image Processing Using Complex Networks
- PMID: 35894027
- PMCID: PMC9332806
- DOI: 10.3390/tomography8040162
A Novel Method for Lung Image Processing Using Complex Networks
Abstract
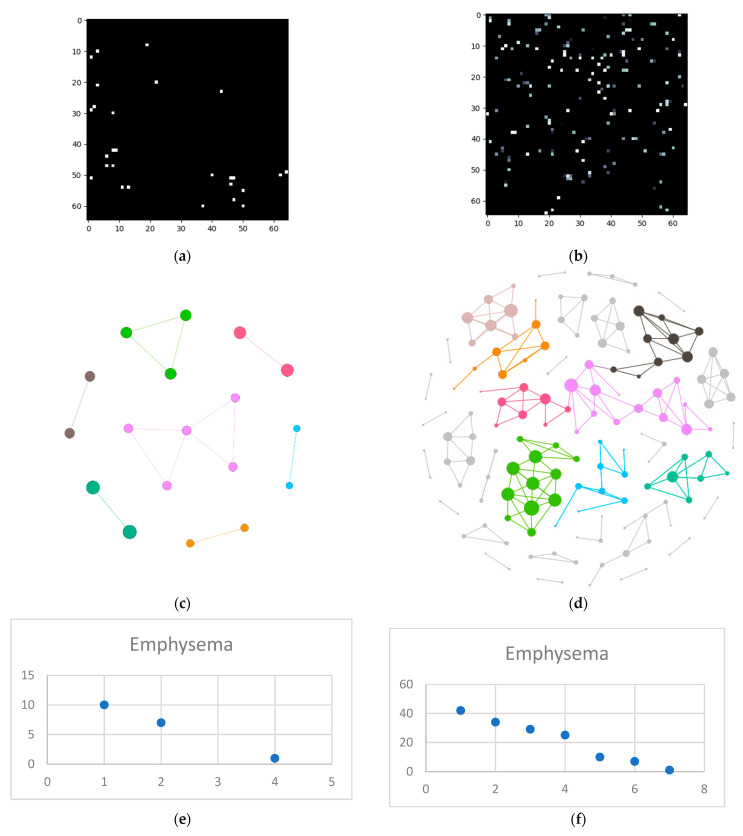
The High-Resolution Computed Tomography (HRCT) detection and diagnosis of diffuse lung disease is primarily based on the recognition of a limited number of specific abnormal findings, pattern combinations or their distributions, as well as anamnesis and clinical information. Since texture recognition has a very high accuracy percentage if a complex network approach is used, this paper aims to implement such a technique customized for diffuse interstitial lung diseases (DILD). The proposed procedure translates HRCT lung imaging into complex networks by taking samples containing a secondary lobule, converting them into complex networks and analyzing them in three dimensions: emphysema, ground glass opacity, and consolidation. This method was evaluated on a 60-patient lot and the results showed a clear, quantifiable difference between healthy and affected lungs. By deconstructing the image on three pathological axes, the method offers an objective way to quantify DILD details which, so far, have only been analyzed subjectively.
Keywords: HRCT; complex networks; diffuse interstitial lung disease; model.
Conflict of interest statement
The authors declare no conflict of interest.
Figures












References
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
