

The Role of Pelvic Floor Muscle Training on Low Anterior Resection Syndrome: A Multicenter Randomized Controlled Trial
- PMID: 35894434
- PMCID: PMC9534049
- DOI: 10.1097/SLA.0000000000005632
The Role of Pelvic Floor Muscle Training on Low Anterior Resection Syndrome: A Multicenter Randomized Controlled Trial
Abstract
Background and objective: Total mesorectal excision (TME) for rectal cancer (RC) often results in significant bowel symptoms, commonly known as low anterior resection syndrome (LARS). Although pelvic floor muscle training (PFMT) is recommended in noncancer populations for treating bowel symptoms, this has been scarcely investigated in RC patients. The objective was to investigate PFMT effectiveness on LARS in patients after TME for RC.
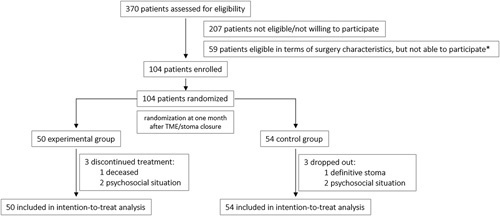
Methods: A multicenter, single-blind prospective randomized controlled trial comparing PFMT (intervention; n=50) versus no PFMT (control; n=54) 1 month following TME/stoma closure was performed. The primary endpoint was the proportion of participants with an improvement in the LARS category at 4 months. Secondary outcomes were: continuous LARS scores, ColoRectal Functioning Outcome scores, Numeric Rating Scale scores, stool diary items, and Short Form 12 scores; all assessed at 1, 4, 6, and 12 months.
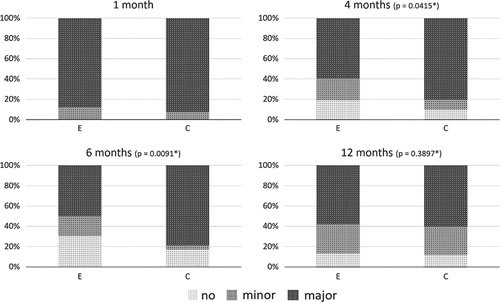
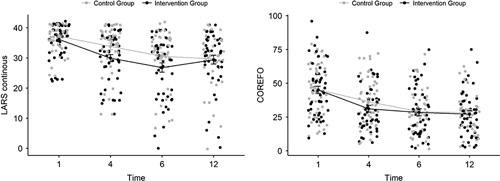
Results: The proportion of participants with an improvement in LARS category was statistically higher after PFMT compared with controls at 4 months (38.3% vs 19.6%; P =0.0415) and 6 months (47.8% vs 21.3%; P =0.0091), but no longer at 12 months (40.0% vs 34.9%; P =0.3897). Following secondary outcomes were significantly lower at 4 months: LARS scores (continuous, P =0.0496), ColoRectal Functioning Outcome scores ( P =0.0369) and frequency of bowel movements ( P =0.0277), solid stool leakage (day, P =0.0241; night, P =0.0496) and the number of clusters ( P =0.0369), derived from the stool diary. No significant differences were found for the Numeric Rating Scale/quality of life scores.
Conclusions: PFMT for bowel symptoms after TME resulted in lower proportions and faster recovery of bowel symptoms up to 6 months after surgery/stoma closure, justifying PFMT as an early, first-line treatment option for bowel symptoms after RC.
Copyright © 2022 The Author(s). Published by Wolters Kluwer Health, Inc.
Conflict of interest statement
The authors report no conflicts of interest.
Figures
References
-
- Borstlap WAA, Deijen CL, den Dulk M, et al. Benchmarking recent national practice in rectal cancer treatment with landmark randomized controlled trials. Colorectal Dis. 2017;19:O219–O231. - PubMed
-
- Bryant CL, Lunniss PJ, Knowles CH, et al. Anterior resection syndrome. Lancet Oncol. 2012;13:e403–e408. - PubMed
-
- Kupsch J, Jackisch T, Matzel KE, et al. Outcome of bowel function following anterior resection for rectal cancer-an analysis using the low anterior resection syndrome (LARS) score. Int J Colorectal Dis. 2018;33:787–798. - PubMed
-
- Keane C, Fearnhead NS, Bordeianou L, et al. International consensus definition of low anterior resection syndrome. Colorectal Dis. 2020;22:331–341. - PubMed
-
- Emmertsen KJ, Laurberg S. Low anterior resection syndrome score: development and validation of a symptom-based scoring system for bowel dysfunction after low anterior resection for rectal cancer. Ann Surg. 2012;255:922–928. - PubMed
