

Pediatric Delirium and All-Cause PICU Readmissions Within 1 Year
- PMID: 35894610
- PMCID: PMC9529805
- DOI: 10.1097/PCC.0000000000003037
Pediatric Delirium and All-Cause PICU Readmissions Within 1 Year
Abstract
Objectives: Delirium in critically ill children is associated with increased in-hospital morbidity and mortality. Little is known about the lingering effects of pediatric delirium in survivors after hospital discharge. The primary objective of this study was to determine whether children with delirium would have a higher likelihood of all-cause PICU readmission within 1 calendar year, when compared with children without delirium.
Design: Retrospective cohort study.
Setting: Tertiary care, mixed PICU at an urban academic medical center.
Patients: Index admissions included all children admitted between September 2014 and August 2015. For each index admission, any readmission occurring within 1 year after PICU discharge was captured.
Intervention: Every child was screened for delirium daily throughout the PICU stay.
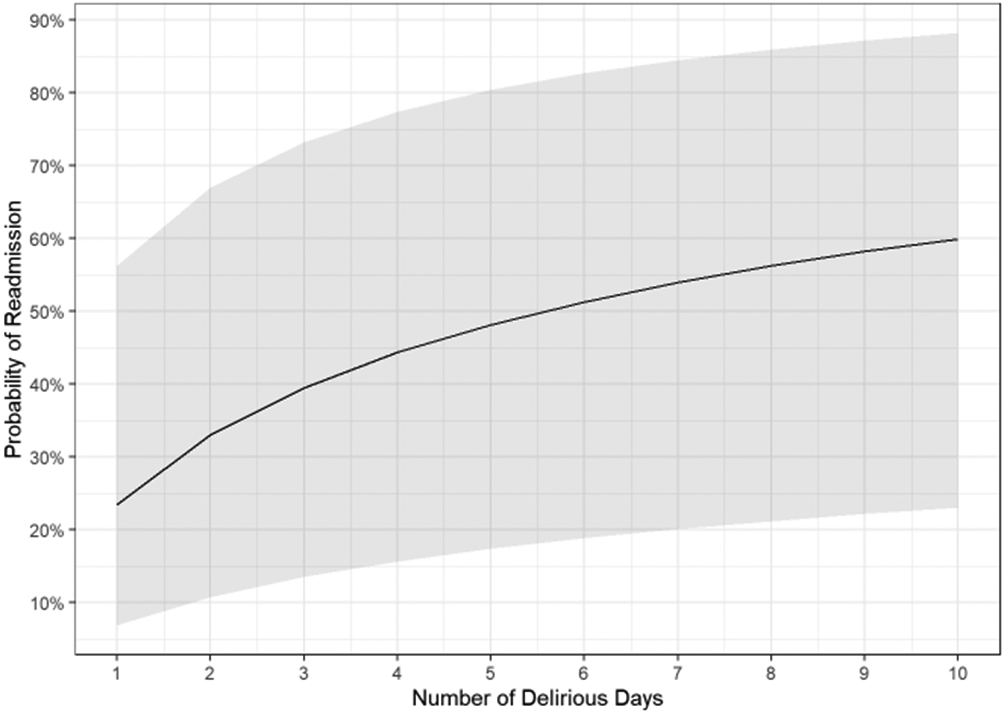
Measurements and main results: Among 1,145 index patients, 166 children (14.5%) were readmitted at least once. Bivariate analyses compared patients readmitted within 1 year of discharge with those not readmitted: complex chronic conditions (CCCs), increased severity of illness, longer PICU length of stay, need for mechanical ventilation, age less than 6 months, and a diagnosis of delirium were all associated with subsequent readmission. A multivariable logistic regression model was constructed to describe adjusted odds ratios for readmission. The primary exposure variable was number of delirium days. After controlling for confounders, critically ill children who experienced greater than 2 delirium days on index admission were more than twice as likely to be readmitted (adjusted odds ratio, 2.2; CI, 1.1-4.4; p = 0.023). A dose-response relationship was demonstrated as children with longer duration of delirium had increased odds of readmission.
Conclusions: In this cohort, delirium duration was an independent risk factor for readmission in critically ill children. Future research is needed to determine if decreasing prevalence of delirium during hospitalization can decrease need for PICU readmission.
Copyright © 2022 by the Society of Critical Care Medicine and the World Federation of Pediatric Intensive and Critical Care Societies.
Conflict of interest statement
Dr. Traube’s institution received funding from the National Institute of Child Health and Human Development and the National Cancer Institute; she received support for article research from the National Institutes of Health. The remaining authors have disclosed that they do not have any potential conflicts of interest.
Figures
Comment in
-
Delirium in the PICU and Hospital Readmission With Delirium Recurrence.Pediatr Crit Care Med. 2022 Oct 1;23(10):843-844. doi: 10.1097/PCC.0000000000003052. Epub 2022 Oct 3. Pediatr Crit Care Med. 2022. PMID: 36190360 No abstract available.
References
-
- American Psychiatric Association: Diagnostic and Statistical Manual of Mental Disorders. Fifth Edition. Arlington, VA, American Psychiatric Association, 2013.
