

Serological findings following the second and third SARS-CoV-2 vaccines in lung transplant recipients
- PMID: 35894705
- PMCID: PMC9311263
- DOI: 10.1002/iid3.646
Serological findings following the second and third SARS-CoV-2 vaccines in lung transplant recipients
Abstract
Introduction: Lung transplant recipients (LuTX) represent a vulnerable population for severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2). Even though many vaccines are already developed, more clinical data need to support effective immunological response in immunocompromised patients.
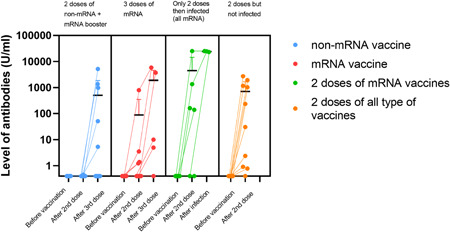
Methods: Stable LuTX recipients with no medical history of coronavirus disease (COVID-19) were enrolled. Currently available messenger RNA (mRNA) (BNT162b2-mRNA, mRNA-1273) and non-mRNA (ChAdOx1, BBIBP-CorV) vaccines were given according to availability, boosters were all mRNA-based. SARS-CoV-2 Spike1 immunoglobulin G (IgG) antibody titer was evaluated before and 2 weeks after second and third dose. Difference between mRNA versus non-mRNA vaccines was assessed.
Results: Forty-one patients (49% men, age 48.4 ± 13.8 years) received two doses of SARS-CoV-2 vaccines: 23 of mRNA, 18 of non-mRNA, and 24/41 (58%) received a third dose. Median 92 months passed since transplantation, and serum level of tacrolimus was median 5.5 ng/ml. Positive serology was found in 37% of all patients after the second dose, 86% had mRNA vaccine. After the third dose, 29% became positive who had no antibody before. Significantly higher level of antibody was found after the second mRNA than non-mRNA vaccines (2.2 vs. 1568.8 U/ml, respectively, p = .002). 6/23 (26%) patients received two doses of mRNA vaccine developed COVID-19 after the second injection in an average of 178 days, half of them recovered, half of them died in intensive care unit (ICU). 3/6 (50%) patients with two doses mRNA and recovered from COVID-19 had significantly higher level of antibody (average 20847.3 U/ml) than without infection. After the booster vaccine, 1/24 (4%) developed infection.
Conclusion: Immunosuppression therapy may induce a weaker SARS-CoV-2 response in LuTX recipients; therefore, third dose is a priority in transplanted patients. The highest antibody level was measured recovering from COVID after two doses. Our data confirm that booster mRNA vaccine could increase antibody levels, even if immunization was started with non-mRNA vaccine.
Keywords: COVID-19; SARS-CoV-2; mRNA vaccine; non-mRNA vaccine; pandemic; third vaccination; transplant; vaccine.
© 2022 The Authors. Immunity, Inflammation and Disease published by John Wiley & Sons Ltd.
Conflict of interest statement
The authors declare no conflicts of interest.
Figures
References
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
