

Do adrenergic alpha-antagonists increase the risk of poor cardiovascular outcomes? A systematic review and meta-analysis
- PMID: 35894772
- PMCID: PMC9715777
- DOI: 10.1002/ehf2.14012
Do adrenergic alpha-antagonists increase the risk of poor cardiovascular outcomes? A systematic review and meta-analysis
Abstract
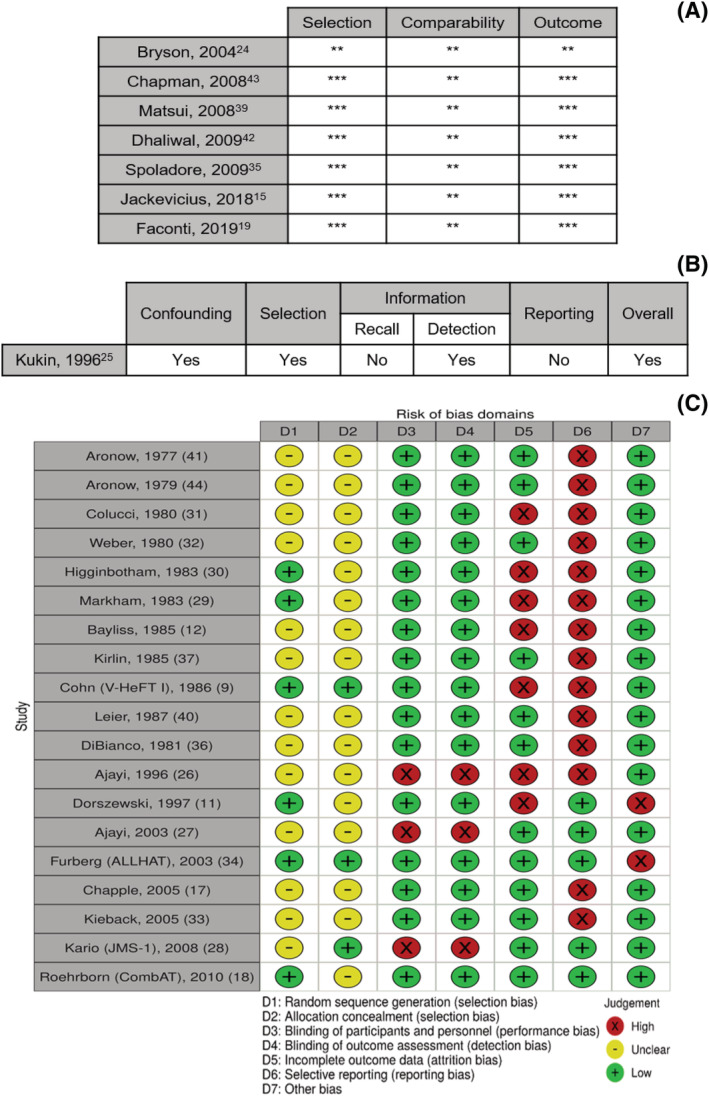
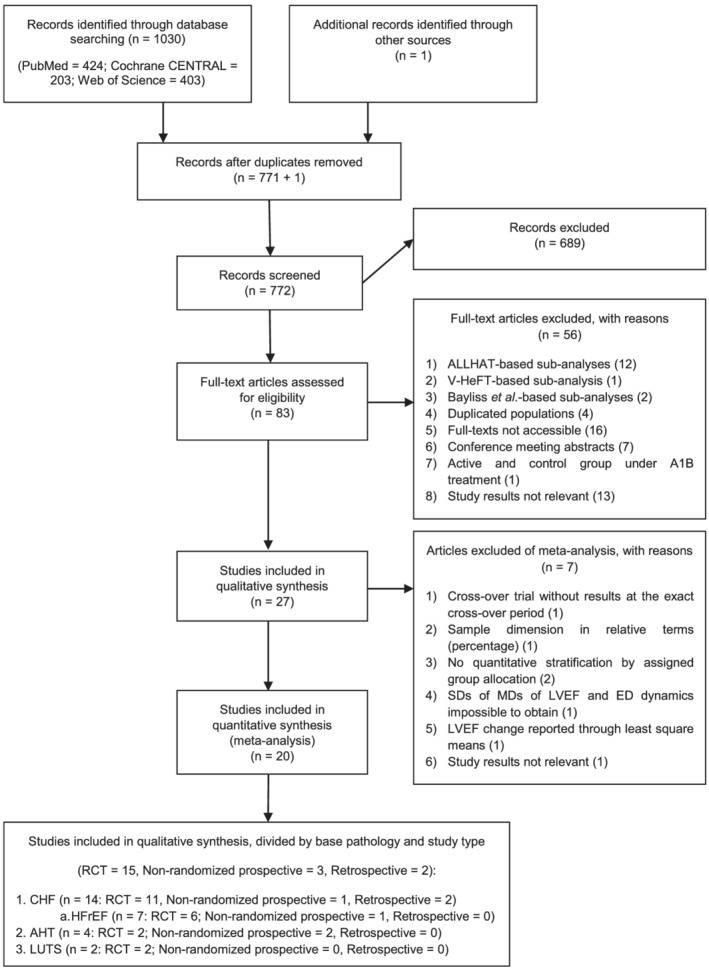
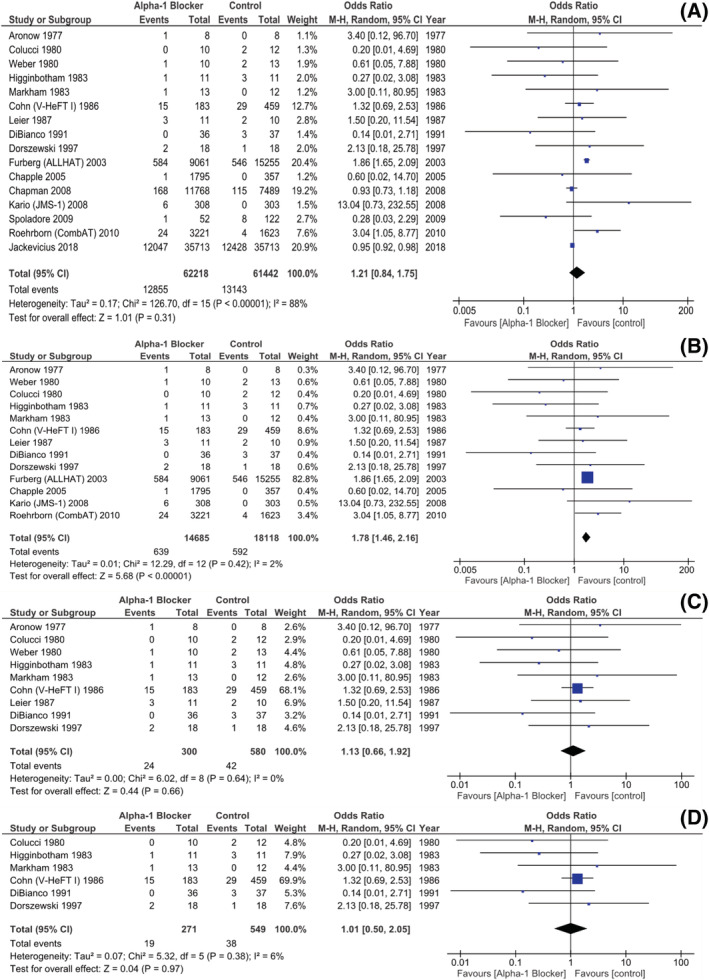
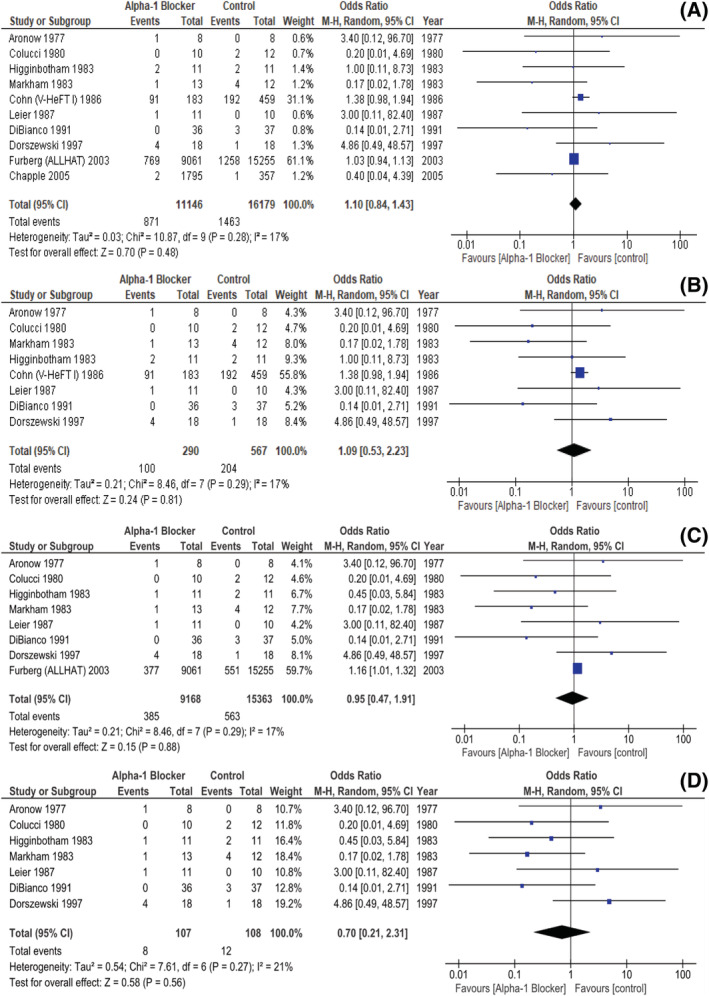
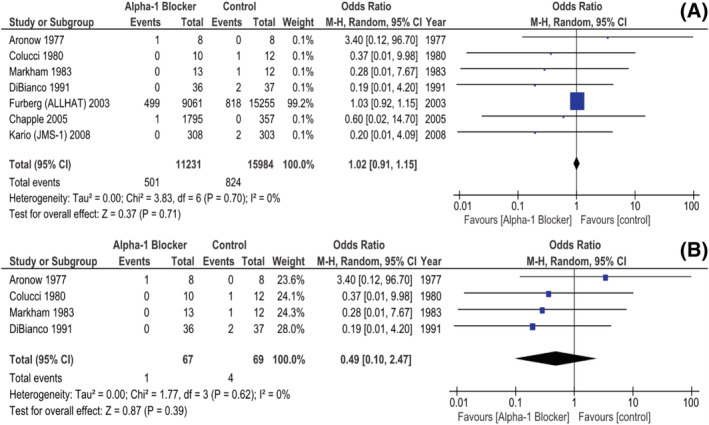
Due to concerns regarding neurohormonal activation and fluid retention, adrenergic alpha-1 receptor antagonists (A1Bs) are generally avoided in the setting of heart disease, namely, symptomatic heart failure (HF) with reduced ejection fraction (HFrEF). However, this contraindication is mainly supported by ancient studies, having recently been challenged by newer ones. We aim to perform a comprehensive meta-analysis aimed at ascertaining the extent to which A1Bs might influence cardiovascular (CV) outcomes. We systematically searched PubMed, Cochrane Central Register of Controlled Trials and Web of Science for both prospective and retrospective studies, published until 1 December 2020, addressing the impact of A1Bs on both clinical outcomes-namely, acute heart failure (AHF), acute coronary syndrome (ACS), CV and all-cause mortality-and on CV surrogate measures, specifically left ventricular ejection fraction (LVEF) and exercise tolerance, by means of exercise duration. Both randomized controlled trials (RCTs) and studies including only HF patients were further investigated separately. Study-specific odds ratios (ORs) and mean differences (MDs) were pooled using traditional meta-analytic techniques, under a random-effects model. A record was registered in PROSPERO database, with the code number CRD42020181804. Fifteen RCTs, three non-randomized prospective and two retrospective studies, encompassing 32 851, 19 287, and 71 600 patients, respectively, were deemed eligible; 62 256 patients were allocated to A1B, on the basis of multiple clinical indications: chronic HF itself [14 studies, with 72 558 patients, including seven studies with 850 HFrEF or HF with mildly reduced ejection fraction (HFmrEF) patients], arterial hypertension (four studies, with 44 184 patients) and low urinary tract symptoms (two studies, with 6996 patients). There were 25 998 AHF events, 1325 ACS episodes, 955 CV deaths and 33 567 all-cause deaths. When considering only RCTs, A1Bs were, indeed, found to increase AHF risk (OR 1.78, [1.46, 2.16] 95% CI, P < 0.00001, i2 2%), although displaying no significant effect on neither ACS nor CV or all-cause mortality rates (OR 1.02, [0.91, 1.15] 95% CI, i2 0%; OR 0.95, [0.47, 1.91] 95% CI, i2 17%; OR 1.1, [0.84, 1.43] 95% CI, i2 17%, respectively). Besides, when only HF patients were evaluated, A1Bs revealed themselves neutral towards not only ACS, CV, and all-cause mortality events (OR 0.49, [0.1, 2.47] 95% CI, i2 0%; OR 0.7, [0.21, 2.31] 95% CI, i2 21%; OR 1.09, [0.53, 2.23] 95% CI, i2 17%, respectively), but also AHF (OR 1.13, [0.66, 1.92] 95% CI, i2 0%). As for HFrEF and HFmrEF, A1Bs were found to exert a similarly inconsequential effect on AHF rates (OR 1.01, [0.5-2.05] 95% CI, i2 6%). Likewise, LVEF was not significantly influenced by A1Bs (MD 1.66, [-2.18, 5.50] 95% CI, i2 58%). Most strikingly, exercise tolerance was higher in those under this drug class (MD 139.16, [65.52, 212.8] 95% CI, P < 0.001, i2 26%). A1Bs do not seem to exert a negative influence on the prognosis of HF-and even of HFrEF-patients, thus contradicting currently held views. These drugs' impact on other major CV outcomes also appear trivial and they may even increment exercise tolerance.
Keywords: Acute coronary syndrome; Adrenergic alpha-antagonists; Exercise tolerance; Heart failure; Left ventricular ejection fraction; Mortality.
© 2022 The Authors. ESC Heart Failure published by John Wiley & Sons Ltd on behalf of European Society of Cardiology.
Conflict of interest statement
José Pedro Sousa, Diogo Mendonça, Rogério Teixeira and Lino Gonçalves have no conflicts of interest, of any nature, to declare. All authors have seen and agree with the contents of the manuscript. We certify that the submission is original work and is not under review at any other publication.
Figures


References
-
- GBD 2017 Disease and Injury Incidence and Prevalence Collaborators . Global, regional, and national incidence, prevalence, and years lived with disability for 354 diseases and injuries for 195 countries and territories, 1990–2017: A systematic analysis for the global burden of disease study 2017. Lancet. 2018; 392: 1789–1858. - PMC - PubMed
-
- Farmakis D, Parissis J, Lekakis J, Filippatos G. Acute heart failure: Epidemiology, risk factors, and prevention. Rev Esp Cardiol (Engl Ed). 2015; 68: 245. - PubMed
-
- McDonagh T, Metra M, Adamo M, Gardner R, Baumbach A, Böhm M, Burri H, Butler J, Čelutkienė J, Chioncel O, Cleland JG. 2021 ESC guidelines for the diagnosis and treatment of acute and chronic heart failure. Eur Heart J. 2021; 42: 3599–3726. - PubMed
-
- Williams B, Mancia G, Spiering W, Rosei E, Azizi M, Burnier M, Clement DL, Coca A, de Simone G, Dominiczak A, Kahan T, Mahfoud F, Redon J, Ruilope L, Zanchetti A, Kerins M, Kjeldsen SE, Kreutz R, Laurent S, Lip GYH, McManus R, Narkiewicz K, Ruschitzka F, Schmieder RE, Shlyakhto E, Tsioufis C, Aboyans V, Desormais I, ESC Scientific Document Group . 2018 ESC/ESH guidelines for the management of arterial hypertension: The task force for the management of arterial hypertension of the European Society of Cardiology (ESC) and the European Society of Hypertension (ESH). Eur Heart J. 2018; 39: 3021–3104.
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
