

Nonoperative vs Operative Management of Uncomplicated Acute Appendicitis: A Systematic Review and Meta-analysis
- PMID: 35895073
- PMCID: PMC9330355
- DOI: 10.1001/jamasurg.2022.2937
Nonoperative vs Operative Management of Uncomplicated Acute Appendicitis: A Systematic Review and Meta-analysis
Erratum in
-
Error in Figures.JAMA Surg. 2023 Aug 1;158(8):892. doi: 10.1001/jamasurg.2023.2493. JAMA Surg. 2023. PMID: 37342047 Free PMC article. No abstract available.
Abstract
Importance: Appendectomy remains the standard of care for uncomplicated acute appendicitis despite several randomized clinical trials pointing to the safety and efficacy of nonoperative management of this disease. A meta-analysis of randomized clinical trials may contribute to the body of evidence and help surgeons select which patients may benefit from surgical and nonsurgical treatment.
Objective: To assess the efficacy and safety of nonoperative management vs appendectomy for acute uncomplicated appendicitis.
Data sources: A systematic review was conducted using indexed sources (Embase and PubMed) to search for published randomized clinical trials in English comparing nonoperative management with appendectomy in adult patients presenting with uncomplicated acute appendicitis. To increase sensitivity, no limits were set for outcomes reported, sex, or year of publication. All nonrandomized or quasi-randomized trials were excluded, and validated primers were used.
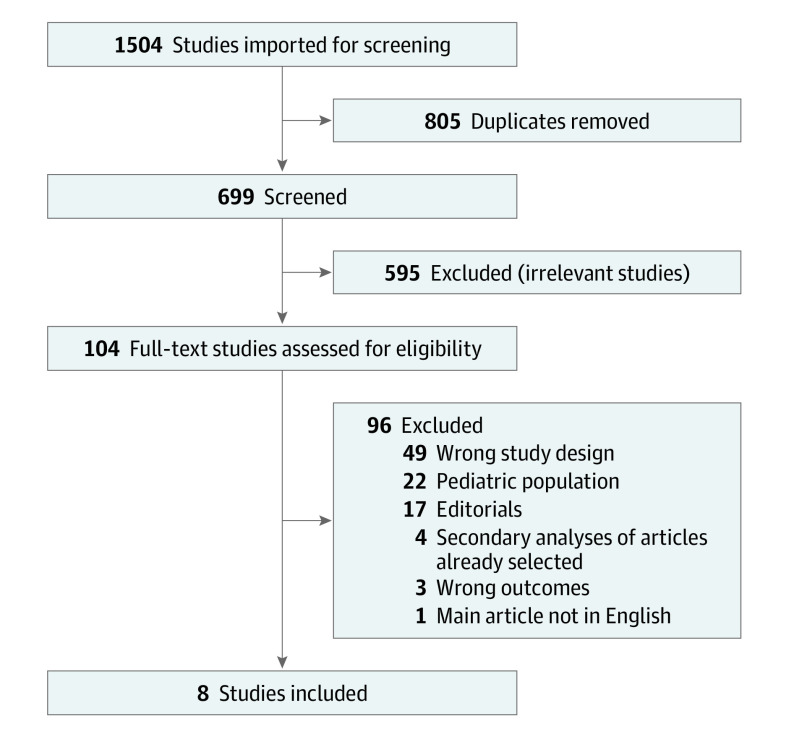
Study selection: Among 1504 studies imported for screening, 805 were duplicates, and 595 were excluded for irrelevancy. A further 96 were excluded after full-text review, mainly owing to wrong study design or inclusion of pediatric populations. Eight studies met the inclusion criteria and were selected for the meta-analysis.
Data extraction and synthesis: Meta-extraction was conducted with independent extraction by multiple reviewers using the Covidence platform for systematic reviews and in accordance with PRISMA guidelines. Data were pooled by a random-effects model.
Main outcomes and measures: Treatment success and major adverse effects at 30 days' follow-up.
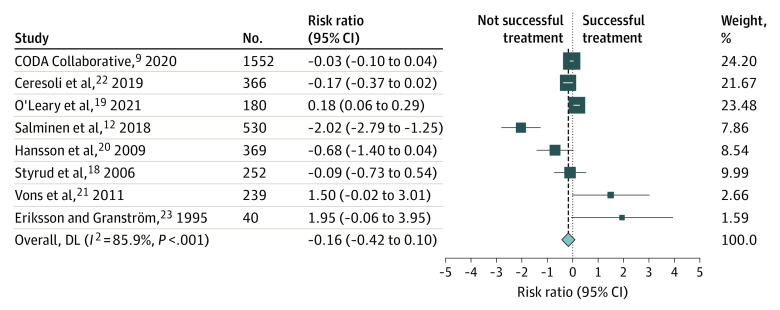
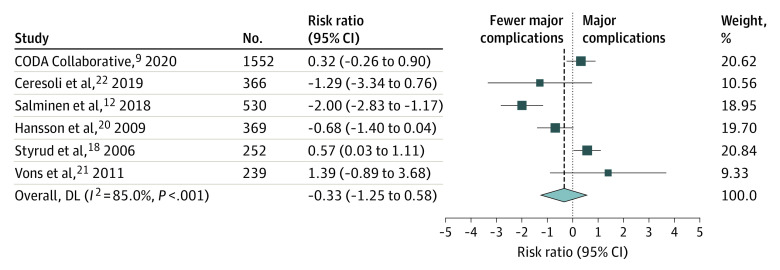
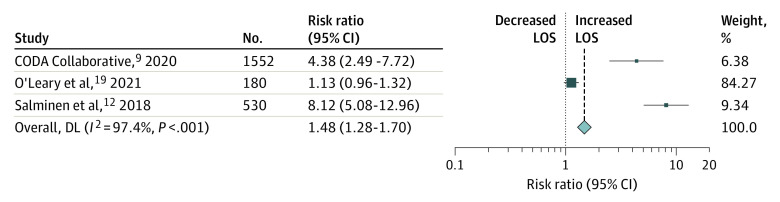
Results: The main outcome (treatment success proportion at 30 days of follow-up) was not significantly different in the operative and nonoperative management cohorts (risk ratio [RR], 0.85; 95% CI, 0.66-1.11). Likewise, the percentage of major adverse effects was similar in both cohorts (RR, 0.72; 95% CI, 0.29-1.79). However, in the nonoperative management group, length of stay was significantly longer (RR, 1.48; 95% CI, 1.26-1.70), and a median cumulative incidence of 18% of recurrent appendicitis was observed.
Conclusions and relevance: These results point to the general safety and efficacy of nonoperative management of uncomplicated acute appendicitis. However, this strategy may be associated with an increase in duration of hospital stay and a higher rate of recurrent appendicitis. This meta-analysis may help inform decision-making in nonoperative management of uncomplicated acute appendicitis.
Conflict of interest statement
Figures
Comment in
-
Management of Acute Uncomplicated Appendicitis.JAMA Surg. 2023 Mar 1;158(3):328-329. doi: 10.1001/jamasurg.2022.6541. JAMA Surg. 2023. PMID: 36515927 No abstract available.
-
Management of Acute Uncomplicated Appendicitis-Reply.JAMA Surg. 2023 Mar 1;158(3):329. doi: 10.1001/jamasurg.2022.6544. JAMA Surg. 2023. PMID: 36515936 No abstract available.
-
Management of Acute Uncomplicated Appendicitis.JAMA Surg. 2023 Mar 1;158(3):328. doi: 10.1001/jamasurg.2022.6538. JAMA Surg. 2023. PMID: 36515963 No abstract available.
References
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
