

Galectin-3 is elevated in CSF and is associated with Aβ deposits and tau aggregates in brain tissue in Alzheimer's disease
- PMID: 35895141
- PMCID: PMC9547798
- DOI: 10.1007/s00401-022-02469-6
Galectin-3 is elevated in CSF and is associated with Aβ deposits and tau aggregates in brain tissue in Alzheimer's disease
Abstract
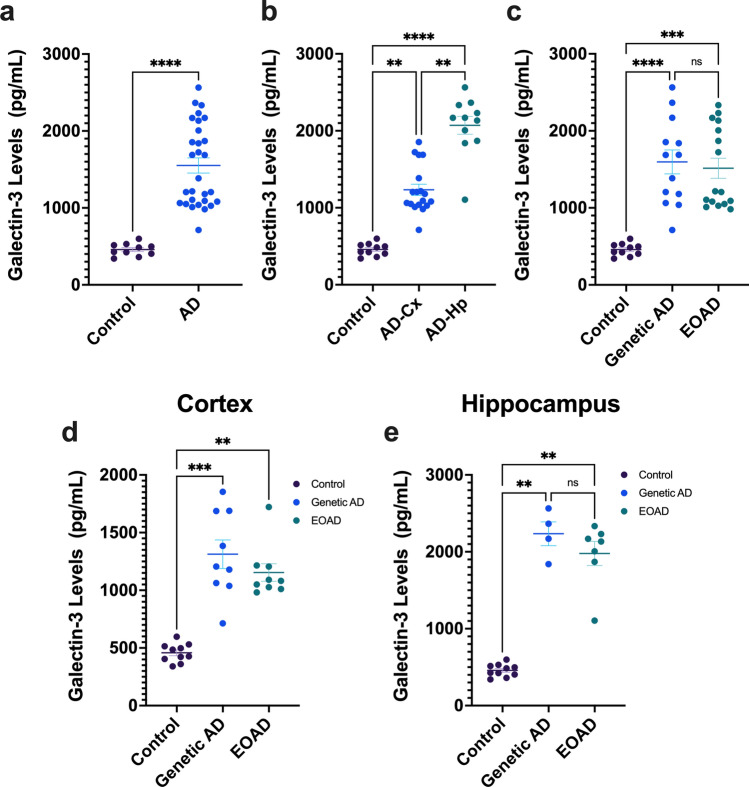
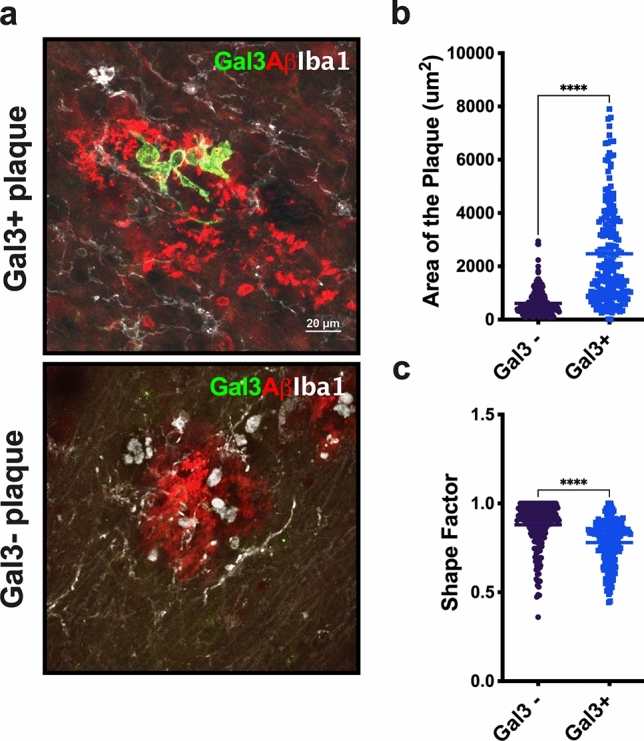
Galectin-3 (Gal-3) is a beta-galactosidase binding protein involved in microglial activation in the central nervous system (CNS). We previously demonstrated the crucial deleterious role of Gal-3 in microglial activation in Alzheimer's disease (AD). Under AD conditions, Gal-3 is primarily expressed by microglial cells clustered around Aβ plaques in both human and mouse brain, and knocking out Gal-3 reduces AD pathology in AD-model mice. To further unravel the importance of Gal-3-associated inflammation in AD, we aimed to investigate the Gal-3 inflammatory response in the AD continuum. First, we measured Gal-3 levels in neocortical and hippocampal tissue from early-onset AD patients, including genetic and sporadic cases. We found that Gal-3 levels were significantly higher in both cortex and hippocampus in AD subjects. Immunohistochemistry revealed that Gal-3+ microglial cells were associated with amyloid plaques of a larger size and more irregular shape and with neurons containing tau-inclusions. We then analyzed the levels of Gal-3 in cerebrospinal fluid (CSF) from AD patients (n = 119) compared to control individuals (n = 36). CSF Gal-3 levels were elevated in AD patients compared to controls and more strongly correlated with tau (p-Tau181 and t-tau) and synaptic markers (GAP-43 and neurogranin) than with amyloid-β. Lastly, principal component analysis (PCA) of AD biomarkers revealed that CSF Gal-3 clustered and associated with other CSF neuroinflammatory markers, including sTREM-2, GFAP, and YKL-40. This neuroinflammatory component was more highly expressed in the CSF from amyloid-β positive (A+), CSF p-Tau181 positive (T+), and biomarker neurodegeneration positive/negative (N+/-) (A + T + N+/-) groups compared to the A + T-N- group. Overall, Gal-3 stands out as a key pathological biomarker of AD pathology that is measurable in CSF and, therefore, a potential target for disease-modifying therapies involving the neuroinflammatory response.
© 2022. The Author(s).
Conflict of interest statement
The authors do not declare any conflict of interest.
Figures





References
-
- Alosco ML, Tripodis Y, Fritts NG, Heslegrave A, Baugh CM, Conneely S, et al. Cerebrospinal fluid tau, Abeta, and sTREM2 in former national football league players: modeling the relationship between repetitive head impacts, microglial activation, and neurodegeneration. Alzheimer’s Dement. 2018;14:1159–1170. doi: 10.1016/j.jalz.2018.05.004. - DOI - PMC - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
