

Endoscopic surveillance alone is feasible and safe in type I gastric neuroendocrine neoplasms less than 10 mm in diameter
- PMID: 35895180
- PMCID: PMC9474380
- DOI: 10.1007/s12020-022-03143-3
Endoscopic surveillance alone is feasible and safe in type I gastric neuroendocrine neoplasms less than 10 mm in diameter
Abstract
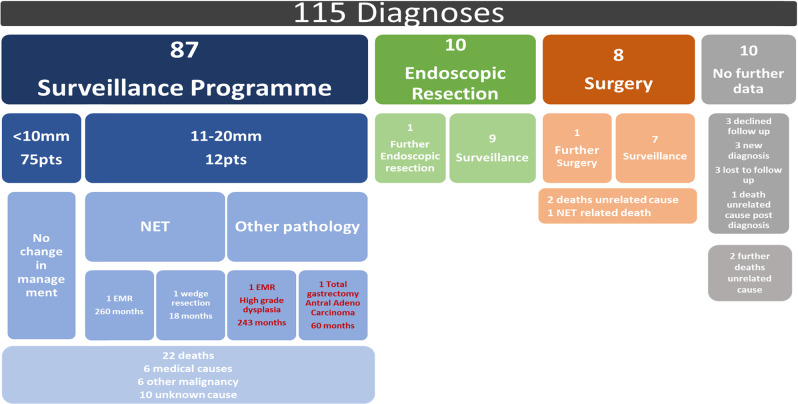
Purpose: Type I gastric neuroendocrine neoplasms (g-NENs) have a low risk of metastasis and a generally favourable prognosis. Patients with small type I g-NENs (≤10 mm) frequently require no treatment, whereas those with larger polyps usually undergo resection. We evaluated the safety and outcomes of endoscopic surveillance after no initial treatment in selected patients with type I g-NENs.
Methods: Retrospective analysis of type I g-NEN patients across two European Neuroendocrine Tumour Society Centers of Excellence 2003-2019.
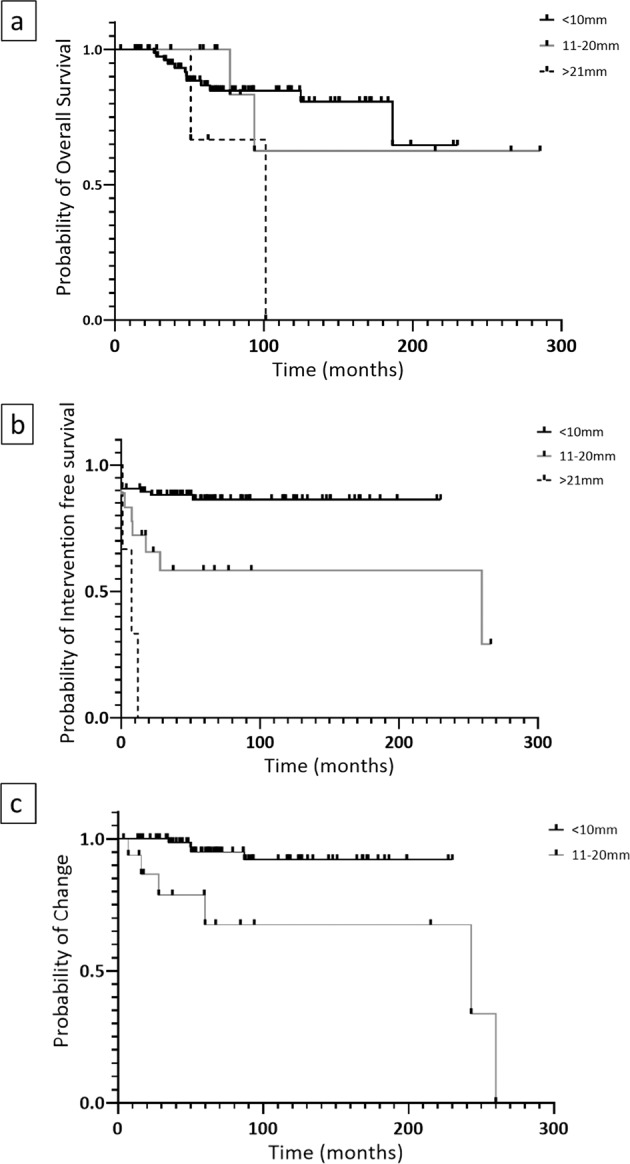
Results: Following initial assessment, 87 of 115 patients with type I g-NEN (75 with polyps ≤10 mm) received no initial treatment and underwent endoscopic surveillance. 79/87 (91%) demonstrated no clinically meaningful change in tumour size or grade over a median 62 month follow up. Only two patients developed NEN progression that required a change in management and two other patients developed gastric adenocarcinoma/high grade dysplasia; all four initially had ≥11 mm g-NENs.
Conclusions: Patients with ≤10 mm type I g-NENs were unlikely to develop clinically significant tumour progression and in most cases, resection was not needed. The endoscopic surveillance interval could therefore potentially be safely increased to every 2-3 years in such patients. However, lifelong surveillance is still advocated due to the additional risk of developing gastric adenocarcinoma.
Keywords: Carcinoid; Endoscopy; Neuroendocrine tumour; Stomach; Surgery; Surveillance.
© 2022. The Author(s).
Conflict of interest statement
K.E. has received consultancy funding from Ipsen. A.R.M. has received consultancy funding from Ipsen. A.L. declares travel and educational support from Ipsen, Pfizer, Bayer, A.A.A., SirtEx, Novartis, Mylan and Delcath, speaker honoraria from Merck, Pfizer, Ipsen, Incyte, A.A.A., Q.E.D., Servier, Astra Zeneca and EISAI, advisory and consultancy honoraria from EISAI, Nutricia Ipsen, Q.E.D., Roche, Servier, Boston Scientific, Albireo Pharma, AstraZeneca, Boehringer Ingelheim and GENFIT, she is a member of the Knowledge Network and NETConnect Initiatives funded by Ipsen. WM has received consultancy funding from Ipsen, Novartis, Pfizer, Merck and B.M.S. Speakers’ Bureau. He has received travel grants from Merck and Ipsen as well as research funding from Nordic, M.S.D. R.H. has received consultancy funding from Ipsen and served on advisory boards for Ipsen. He has received conference attendance support. M.M.N. received research grant support from Servier, Ipsen, and NuCana. She has received travel and accommodation support from Bayer and Ipsen and speaker honoraria from Pfizer, Ipsen, NuCana, Mylan and Advanced Accelerator Applications (UK & Ireland) Ltd. She has served on advisory boards for Celgene, Ipsen, Sirtex, Baxalta, Incyte and Astra Zeneca; all outside of the scope of this work. J.W.V. reports personal fees from Agios, AstraZeneca, Baxter, Genoscience Pharma, Hutchison Medipharma, Imaging Equipment Ltd (AAA), Incyte, Ipsen, Mundipharma E.D.O., Mylan, Q.E.D., Servier, Sirtex, Zymeworks; and grants, personal fees, and non-financial support from NuCana, outside the submitted work. D.M.P. has received consultancy funding from Ipsen, Advanced Accelerator Applications and Mayoly Spindler laboratories and research funding from Trio Medicines Ltd. None of the other authors have any conflicts of interest to declare.
Figures
Similar articles
-
Advances in Endoscopic Diagnosis and Treatment of Gastric Neuroendocrine Neoplasms.Dig Dis Sci. 2024 Jan;69(1):27-35. doi: 10.1007/s10620-023-08180-0. Epub 2023 Nov 16. Dig Dis Sci. 2024. PMID: 37971578 Review.
-
Is local excision sufficient in selected grade 1 or 2 type III gastric neuroendocrine neoplasms?Endocrine. 2021 Nov;74(2):421-429. doi: 10.1007/s12020-021-02775-1. Epub 2021 Jun 12. Endocrine. 2021. PMID: 34120313
-
[Consensus and controversy on subtype classification of gastric neuroendocrine neoplasms].Zhonghua Wei Chang Wai Ke Za Zhi. 2017 Sep 25;20(9):977-981. Zhonghua Wei Chang Wai Ke Za Zhi. 2017. PMID: 28900986 Chinese.
-
Modern Management of Gastric Neuroendocrine Neoplasms.Curr Treat Options Oncol. 2024 Sep;25(9):1137-1152. doi: 10.1007/s11864-024-01207-2. Epub 2024 Jul 31. Curr Treat Options Oncol. 2024. PMID: 39083164 Review.
-
Selective Resection of Type 1 Gastric Neuroendocrine Neoplasms and the Risk of Progression in an Endoscopic Surveillance Programme.Dig Surg. 2021;38(1):38-45. doi: 10.1159/000510962. Epub 2020 Dec 1. Dig Surg. 2021. PMID: 33260173
Cited by
-
Advances in Endoscopic Diagnosis and Treatment of Gastric Neuroendocrine Neoplasms.Dig Dis Sci. 2024 Jan;69(1):27-35. doi: 10.1007/s10620-023-08180-0. Epub 2023 Nov 16. Dig Dis Sci. 2024. PMID: 37971578 Review.
-
[Management of Type 1 Gastric Neuroendocrine Tumors Less than 10 mm in Diameter].Korean J Helicobacter Up Gastrointest Res. 2023 Mar;23(1):76-78. doi: 10.7704/kjhugr.2022.0065. Epub 2023 Mar 9. Korean J Helicobacter Up Gastrointest Res. 2023. PMID: 40503382 Free PMC article. Korean. No abstract available.
-
Therapeutic Challenges for Gastric Neuroendocrine Neoplasms: Take It or Leave It?Medicina (Kaunas). 2023 Oct 1;59(10):1757. doi: 10.3390/medicina59101757. Medicina (Kaunas). 2023. PMID: 37893475 Free PMC article. Review.
-
Type 2 and type 3 gastric neuroendocrine tumors have high risk of lymph node metastasis: Systematic review and meta-analysis.Dig Endosc. 2025 Aug;37(8):834-843. doi: 10.1111/den.15026. Epub 2025 Apr 1. Dig Endosc. 2025. PMID: 40170116 Free PMC article. Review.
-
Unraveling the Mysteries of Autoimmune Gastritis.Turk J Gastroenterol. 2024 Nov 25;36(3):135-144. doi: 10.5152/tjg.2024.24563. Turk J Gastroenterol. 2024. PMID: 39632655 Free PMC article. Review.
References
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
