

Primary cutaneous peripheral T-cell lymphomas with a T-follicular helper phenotype: an integrative clinical, pathological and molecular case series study
- PMID: 35895386
- PMCID: PMC10087773
- DOI: 10.1111/bjd.21791
Primary cutaneous peripheral T-cell lymphomas with a T-follicular helper phenotype: an integrative clinical, pathological and molecular case series study
Abstract
Background: Primary cutaneous peripheral T-cell lymphomas with a T-follicular helper phenotype (pcTFH-PTCL) are poorly characterized, and often compared to, but not corresponding with, mycosis fungoides (MF), Sézary syndrome, primary cutaneous CD4+ lymphoproliferative disorder, and skin manifestations of angioimmunoblastic T-cell lymphomas (AITL).
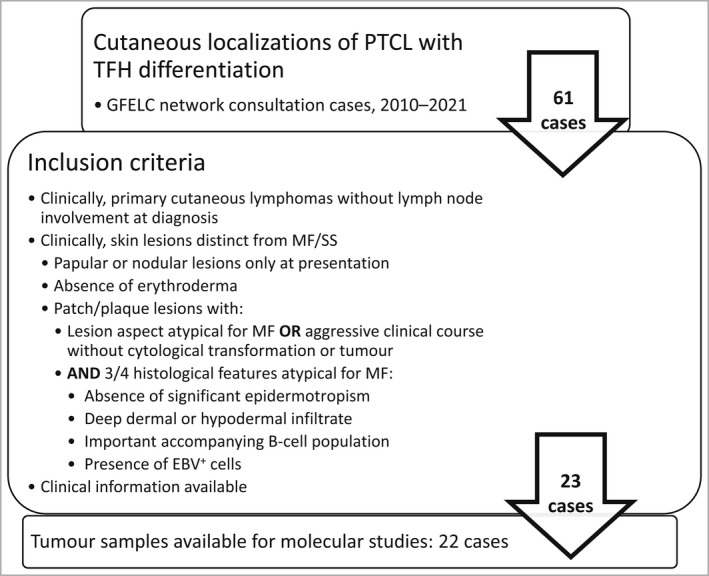
Objectives: We describe the clinicopathological features of pcTFH-PTCL in this original series of 23 patients, and also characterize these cases molecularly.
Methods: Clinical and histopathological data of the selected patients were reviewed. Patient biopsy samples were also analysed by targeted next-generation sequencing.
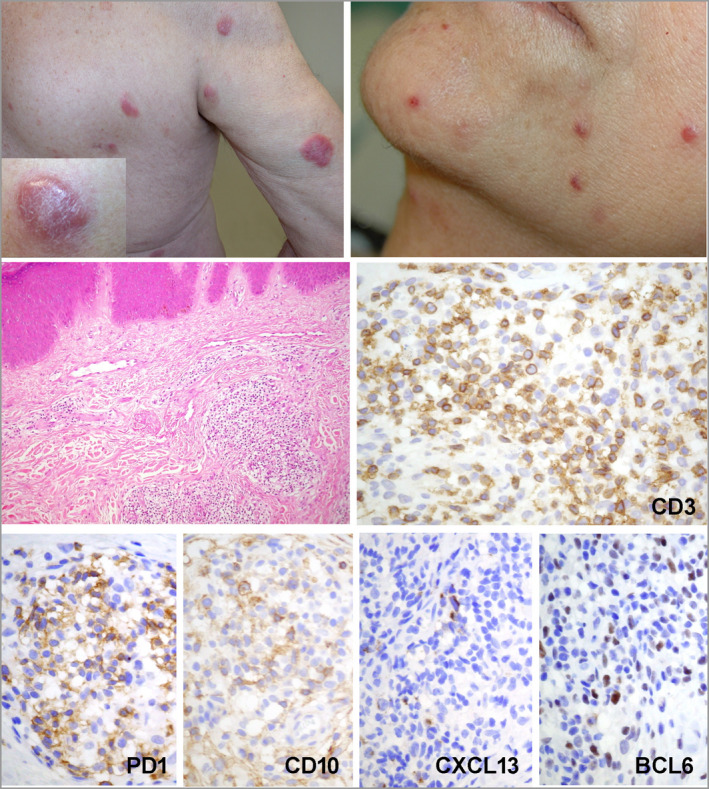
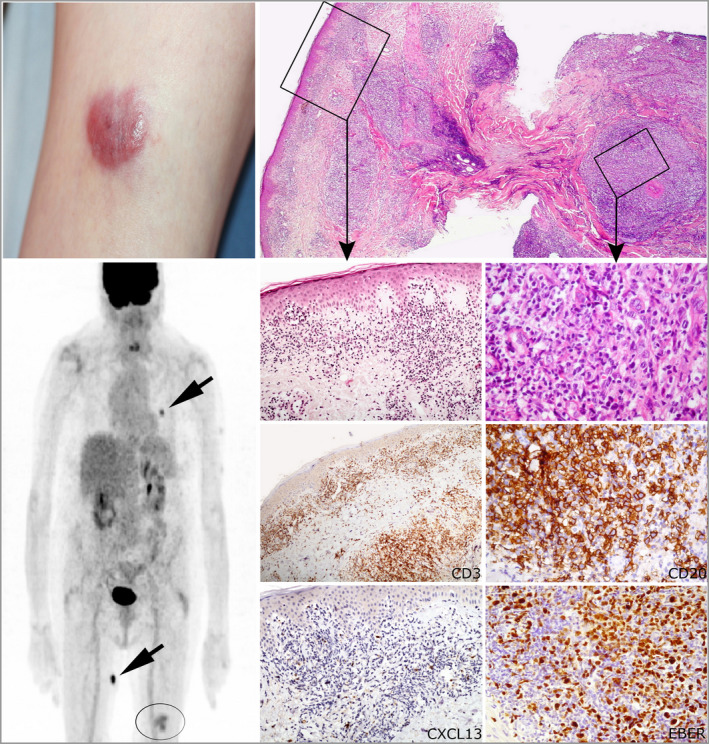
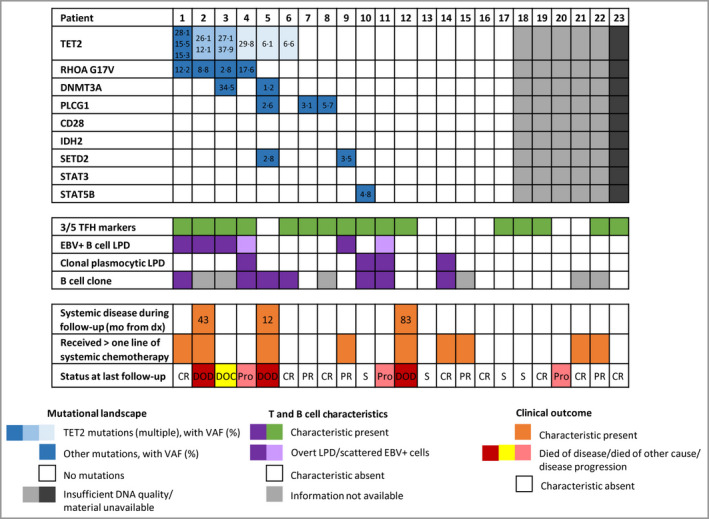
Results: All patients (15 men, eight women; median age 66 years) presented with skin lesions, without systemic disease. Most were stage T3b, with nodular (n = 16), papular (n = 6) or plaque (atypical for MF, n = 1) lesions. Three (13%) developed systemic disease and died of lymphoma. Nine (39%) patients received more than one line of chemotherapy. Histologically, the lymphomas were CD4+ T-cell proliferations, usually dense and located in the deep dermis (n = 14, 61%), with the expression of at least two TFH markers (CD10, CXCL13, PD1, ICOS, BCL6), including three markers in 16 cases (70%). They were associated with a variable proportion of B cells. Eight patients were diagnosed with an associated B-cell lymphoproliferative disorder (LPD) on biopsy, including Epstein-Barr virus (EBV)-positive diffuse large B-cell lymphoma (n = 3), EBV+ LPD (n = 1) and monotypic plasma cell LPD (n = 4). Targeted sequencing showed four patients to have a mutated TET2-RHOAG17V association (as frequently seen in AITL) and another a TET2/DNMT3A/PLCG1/SETD2 mutational profile. The latter patient, one with a TET2-RHOA association, and one with no detected mutations, developed systemic disease and died. Five other patients showed isolated mutations in TET2 (n = 1), PLCG1 (n = 2), SETD2 (n = 1) or STAT5B (n = 1).
Conclusions: Patients with pcTFH-PTCL have pathological and genetic features that overlap with those of systemic lymphoma of TFH derivation. Clinically, most remained confined to the skin, with only three patients showing systemic spread and death. Whether pcTFH-PTCL should be integrated as a new subgroup of TFH lymphomas in future classifications is still a matter of debate. What is already known about this topic? There is a group of cutaneous lymphomas that express T-follicular helper (TFH) markers that do not appear to correspond to existing World Health Organization diagnostic entities. These include mycosis fungoides, Sézary syndrome, or primary cutaneous CD4+ small/medium-sized T-cell lymphoproliferative disorder or cutaneous extensions of systemic peripheral T-cell lymphomas (PTCL) with TFH phenotype. What does this study add? This is the first large original series of patients with a diagnosis of primary cutaneous PTCL with a TFH phenotype (pcTFH-PTCL) to be molecularly characterized. pcTFH-PTCL may be a standalone group of cutaneous lymphomas with clinicopathological and molecular characteristics that overlap with those of systemic TFH lymphomas, such as angioimmunoblastic T-cell lymphoma, and does not belong to known diagnostic groups of cutaneous lymphoma. This has an impact on the treatment and follow-up of patients; the clinical behaviour needs to be better clarified in further studies to tailor patient management.
© 2022 The Authors. British Journal of Dermatology published by John Wiley & Sons Ltd on behalf of British Association of Dermatologists.
Conflict of interest statement
The authors have no conflicts of interest to declare.
Figures
Comment in
-
Follicular T helper cells and cutaneous T-cell lymphomas.Br J Dermatol. 2022 Dec;187(6):841-842. doi: 10.1111/bjd.21839. Epub 2022 Aug 31. Br J Dermatol. 2022. PMID: 36045612 No abstract available.
Similar articles
-
Expression of T-follicular helper markers in sequential biopsies of progressive mycosis fungoides and other primary cutaneous T-cell lymphomas.Am J Dermatopathol. 2015 Feb;37(2):115-21. doi: 10.1097/DAD.0000000000000258. Am J Dermatopathol. 2015. PMID: 25406852
-
Markers of Follicular Helper T Cells Are Occasionally Expressed in T-Cell or Histiocyte-Rich Large B-Cell Lymphoma, Classic Hodgkin Lymphoma, and Atypical Paracortical HyperplasiaA Diagnostic Pitfall For T-Cell Lymphomas of T Follicular Helper Origin.Am J Clin Pathol. 2021 Aug 4;156(3):409-426. doi: 10.1093/ajcp/aqaa249. Am J Clin Pathol. 2021. PMID: 33624021
-
[Analysis of clinicopathological and molecular abnormalities of angioimmunoblastic T-cell lymphoma].Beijing Da Xue Xue Bao Yi Xue Ban. 2023 Jun 18;55(3):521-529. doi: 10.19723/j.issn.1671-167X.2023.03.019. Beijing Da Xue Xue Bao Yi Xue Ban. 2023. PMID: 37291929 Free PMC article. Chinese.
-
Update on peripheral T-cell lymphomas with T-helper phenotype: Are there too many subtypes?Semin Diagn Pathol. 2020 Jan;37(1):24-31. doi: 10.1053/j.semdp.2019.12.005. Epub 2019 Dec 17. Semin Diagn Pathol. 2020. PMID: 31870687 Review.
-
Primary cutaneous T-cell lymphoma (mycosis fungoides and Sézary syndrome): part I. Diagnosis: clinical and histopathologic features and new molecular and biologic markers.J Am Acad Dermatol. 2014 Feb;70(2):205.e1-16; quiz 221-2. doi: 10.1016/j.jaad.2013.07.049. J Am Acad Dermatol. 2014. PMID: 24438969 Review.
Cited by
-
Primary cutaneous T-follicular helper lymphoma.EJHaem. 2023 Jul 31;4(4):1176-1178. doi: 10.1002/jha2.737. eCollection 2023 Nov. EJHaem. 2023. PMID: 38024630 Free PMC article. No abstract available.
-
Update on primary cutaneous T-cell lymphomas rare subtypes.Dermatol Reports. 2024 May 7;16(Suppl 2):9961. doi: 10.4081/dr.2024.9961. eCollection 2024 May 7. Dermatol Reports. 2024. PMID: 39295878 Free PMC article. Review.
-
Skin manifestations uncover underlying Follicular helper T-cell lymphoma, angioimmunoblastic-type in an immunosuppressed patient.Virchows Arch. 2025 Sep 3. doi: 10.1007/s00428-025-04244-w. Online ahead of print. Virchows Arch. 2025. PMID: 40900230
-
mAb14, a Monoclonal Antibody against Cell Surface PCNA: A Potential Tool for Sezary Syndrome Diagnosis and Targeted Immunotherapy.Cancers (Basel). 2023 Sep 4;15(17):4421. doi: 10.3390/cancers15174421. Cancers (Basel). 2023. PMID: 37686697 Free PMC article.
-
Cutaneous T-cell lymphomas: 2023 update on diagnosis, risk-stratification, and management.Am J Hematol. 2023 Jan;98(1):193-209. doi: 10.1002/ajh.26760. Epub 2022 Oct 20. Am J Hematol. 2023. PMID: 36226409 Free PMC article.
References
-
- Swerdlow S, Campo E, Jaffe ES et al. WHO classification of tumours of haematopoietic and lymphoid tissues. Revised 4th edition. Lyon: International Agency for Research on Cancer, 2017; 585.
-
- Leclaire Alirkilicarslan A, Dupuy A, Pujals A et al. Expression of TFH markers and detection of RHOA p.G17V and IDH2 p.R172K/S mutations in cutaneous localizations of angioimmunoblastic T‐cell lymphomas. Am J Surg Pathol 2017; 41:1581–92. - PubMed
-
- Buder K, Poppe LM, Bröcker EB et al. Primary cutaneous follicular helper T‐cell lymphoma: diagnostic pitfalls of this new lymphoma subtype. J Cutan Pathol 2013; 40:903–8. - PubMed
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
