

Burosumab Treatment for Autosomal Recessive Hypophosphatemic Rickets Type 1 (ARHR1)
- PMID: 35896139
- PMCID: PMC9516063
- DOI: 10.1210/clinem/dgac433
Burosumab Treatment for Autosomal Recessive Hypophosphatemic Rickets Type 1 (ARHR1)
Abstract
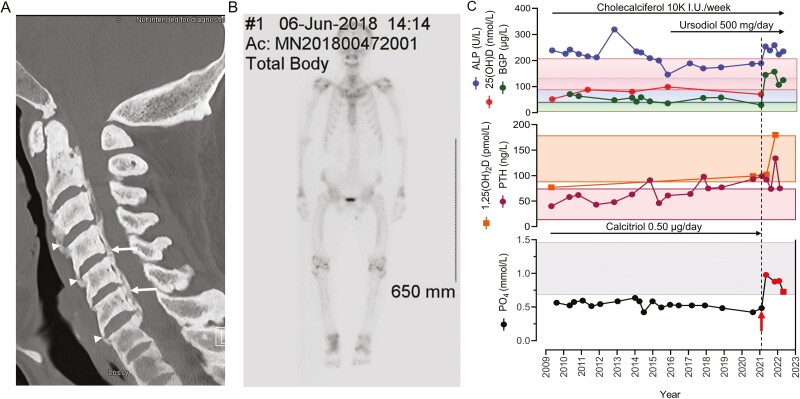
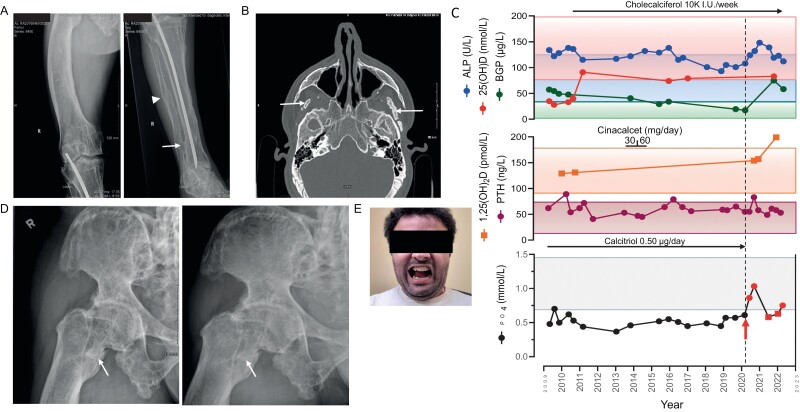
Context: Autosomal recessive hypophosphatemic rickets (ARHR) are rare, heritable renal phosphate-wasting disorders that arise from overexpression of the bone-derived phosphaturic hormone fibroblast growth factor 23 (FGF23) leading to impaired bone mineralization (rickets and osteomalacia). Inactivating mutations of Dentin matrix protein 1 (DMP1) give rise to ARHR type 1 (ARHR1). Short stature, prominent bowing of the legs, fractures/pseudofractures, and severe enthesopathy are prominent in this patient population. Traditionally, treatment consists of oral phosphate replacement and the addition of calcitriol but this approach is limited by modest efficacy and potential renal and gastrointestinal side effects.
Objective: The advent of burosumab (Crysvita), a fully humanized monoclonal antibody to FGF23 for the treatment of X-linked hypophosphatemia and tumor-induced osteomalacia, offers a unique opportunity to evaluate its safety and efficacy in patients with ARHR1.
Results: Monthly administration of burosumab to 2 brothers afflicted with the disorder resulted in normalization of serum phosphate, healing of pseudofracture, diminished fatigue, less bone pain, and reduced incapacity arising from the extensive enthesopathy and soft tissue fibrosis/calcification that characterizes this disorder. No adverse effects were reported following burosumab administration.
Conclusion: The present report highlights the beneficial biochemical and clinical outcomes associated with the use of burosumab in patients with ARHR1.
Keywords: FGF23; burosumab; hypophosphatemic rickets; osteomalacia; pseudofractures.
© The Author(s) 2022. Published by Oxford University Press on behalf of the Endocrine Society. All rights reserved. For permissions, please e-mail: journals.permissions@oup.com.
Figures
Similar articles
-
Pathogenic role of Fgf23 in Dmp1-null mice.Am J Physiol Endocrinol Metab. 2008 Aug;295(2):E254-61. doi: 10.1152/ajpendo.90201.2008. Epub 2008 Jun 17. Am J Physiol Endocrinol Metab. 2008. PMID: 18559986 Free PMC article.
-
Safety and efficacy of burosumab in improving phosphate metabolism, bone health, and quality of life in adolescents with X-linked hypophosphatemic rickets.Eur J Med Genet. 2024 Aug;70:104958. doi: 10.1016/j.ejmg.2024.104958. Epub 2024 Jun 29. Eur J Med Genet. 2024. PMID: 38950880
-
New Therapies for Hypophosphatemia-Related to FGF23 Excess.Calcif Tissue Int. 2021 Jan;108(1):143-157. doi: 10.1007/s00223-020-00705-3. Epub 2020 Jun 5. Calcif Tissue Int. 2021. PMID: 32504139 Review.
-
Effects of Burosumab Treatment on Two Siblings with X-Linked Hypophosphatemia. Case Report and Literature Review.Genes (Basel). 2022 Aug 4;13(8):1392. doi: 10.3390/genes13081392. Genes (Basel). 2022. PMID: 36011303 Free PMC article. Review.
-
FGF23 and Hypophosphatemic Rickets/Osteomalacia.Curr Osteoporos Rep. 2021 Dec;19(6):669-675. doi: 10.1007/s11914-021-00709-4. Epub 2021 Nov 10. Curr Osteoporos Rep. 2021. PMID: 34755323 Review.
Cited by
-
Inherited phosphate and pyrophosphate disorders: New insights and novel therapies changing the oral health landscape.J Am Dent Assoc. 2024 Nov;155(11):912-925. doi: 10.1016/j.adaj.2024.05.016. Epub 2024 Aug 10. J Am Dent Assoc. 2024. PMID: 39127957 Review.
-
Fibroblast Growth Factors: Roles and Emerging Therapeutic Applications.Curr Drug Targets. 2025;26(8):551-570. doi: 10.2174/0113894501351461250301072444. Curr Drug Targets. 2025. PMID: 40051360 Review.
-
Mineral Metabolism in Children: Interrelation between Vitamin D and FGF23.Int J Mol Sci. 2023 Apr 3;24(7):6661. doi: 10.3390/ijms24076661. Int J Mol Sci. 2023. PMID: 37047636 Free PMC article. Review.
-
FGF23 directly inhibits osteoprogenitor differentiation in Dmp1-knockout mice.JCI Insight. 2023 Dec 22;8(24):e156850. doi: 10.1172/jci.insight.156850. JCI Insight. 2023. PMID: 37943605 Free PMC article.
-
One half-century of advances in the evaluation and management of disorders of bone and mineral metabolism in children and adolescents.J Pediatr Endocrinol Metab. 2023 Jan 13;36(2):105-118. doi: 10.1515/jpem-2022-0624. Print 2023 Feb 23. J Pediatr Endocrinol Metab. 2023. PMID: 36636022 Free PMC article. Review.
References
-
- Fisher LW, Fedarko NS. Six genes expressed in bones and teeth encode the current members of the SIBLING family of proteins. Connect Tissue Res. 2003;44(Suppl 1):33-40. - PubMed
Publication types
MeSH terms
Substances
Supplementary concepts
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
