

Short-Term Changes in Serum Potassium and the Risk of Subsequent Vascular Events and Mortality: Results from a Randomized Controlled Trial of ACE Inhibitors
- PMID: 35896277
- PMCID: PMC9435974
- DOI: 10.2215/CJN.00180122
Short-Term Changes in Serum Potassium and the Risk of Subsequent Vascular Events and Mortality: Results from a Randomized Controlled Trial of ACE Inhibitors
Abstract
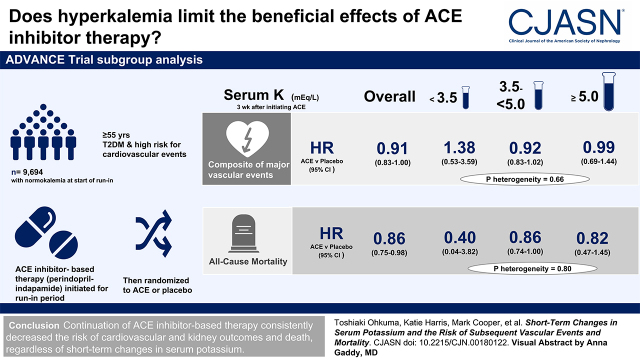
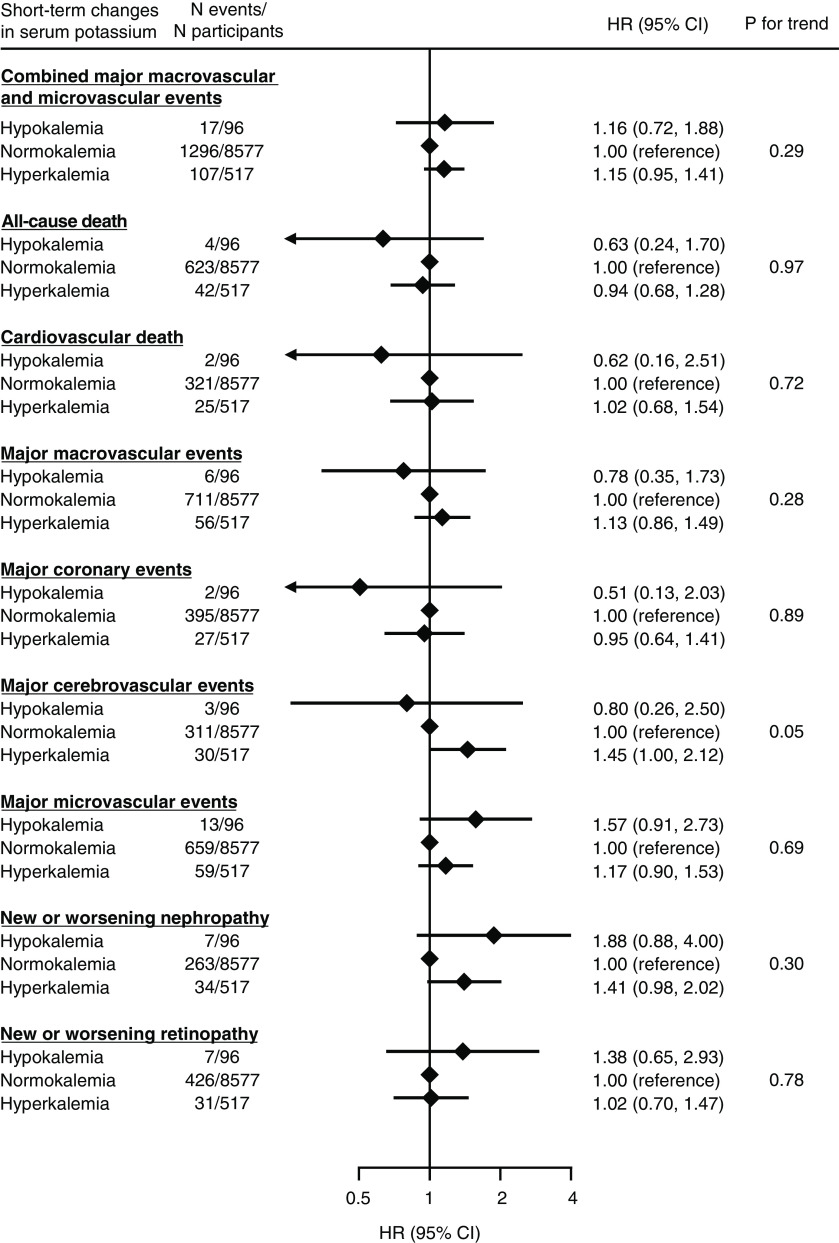
Background and objectives: Hyperkalemia after starting renin-angiotensin system inhibitors has been shown to be subsequently associated with a higher risk of cardiovascular and kidney outcomes. However, whether to continue or discontinue the drug after hyperkalemia remains unclear.
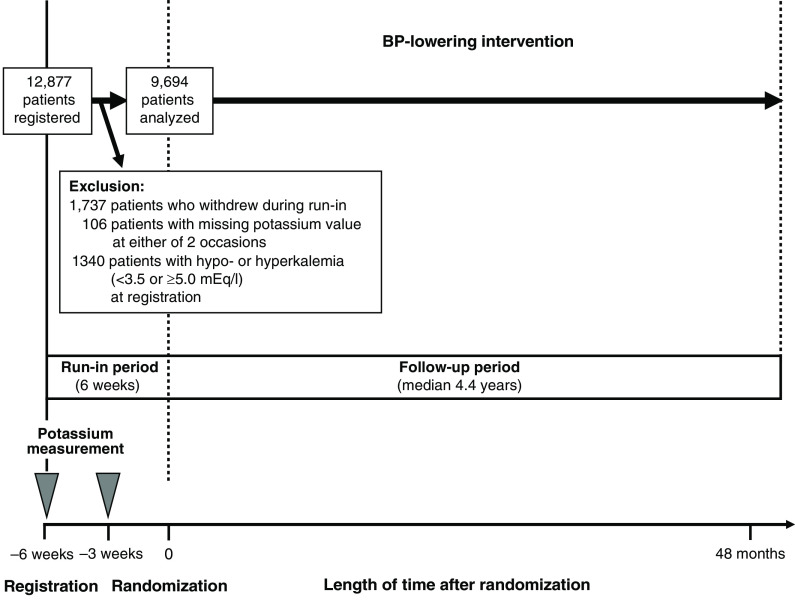
Design, setting, participants, & measurements: Data came from the Action in Diabetes and Vascular Disease: Preterax and Diamicron Modified Release Controlled Evaluation (ADVANCE) trial, which included a run-in period where all participants initiated angiotensin-converting enzyme inhibitor-based therapy (a fixed combination of perindopril and indapamide). The study population was taken as patients with type 2 diabetes with normokalemia (serum potassium of 3.5 to <5.0 mEq/L) at the start of run-in. Potassium was remeasured 3 weeks later when a total of 9694 participants were classified into hyperkalemia (≥5.0 mEq/L), normokalemia, and hypokalemia (<3.5 mEq/L) groups. After run-in, patients were randomized to continuation of the angiotensin-converting enzyme inhibitor-based therapy or placebo; major macrovascular, microvascular, and mortality outcomes were analyzed using Cox regression during the following 4.4 years (median).
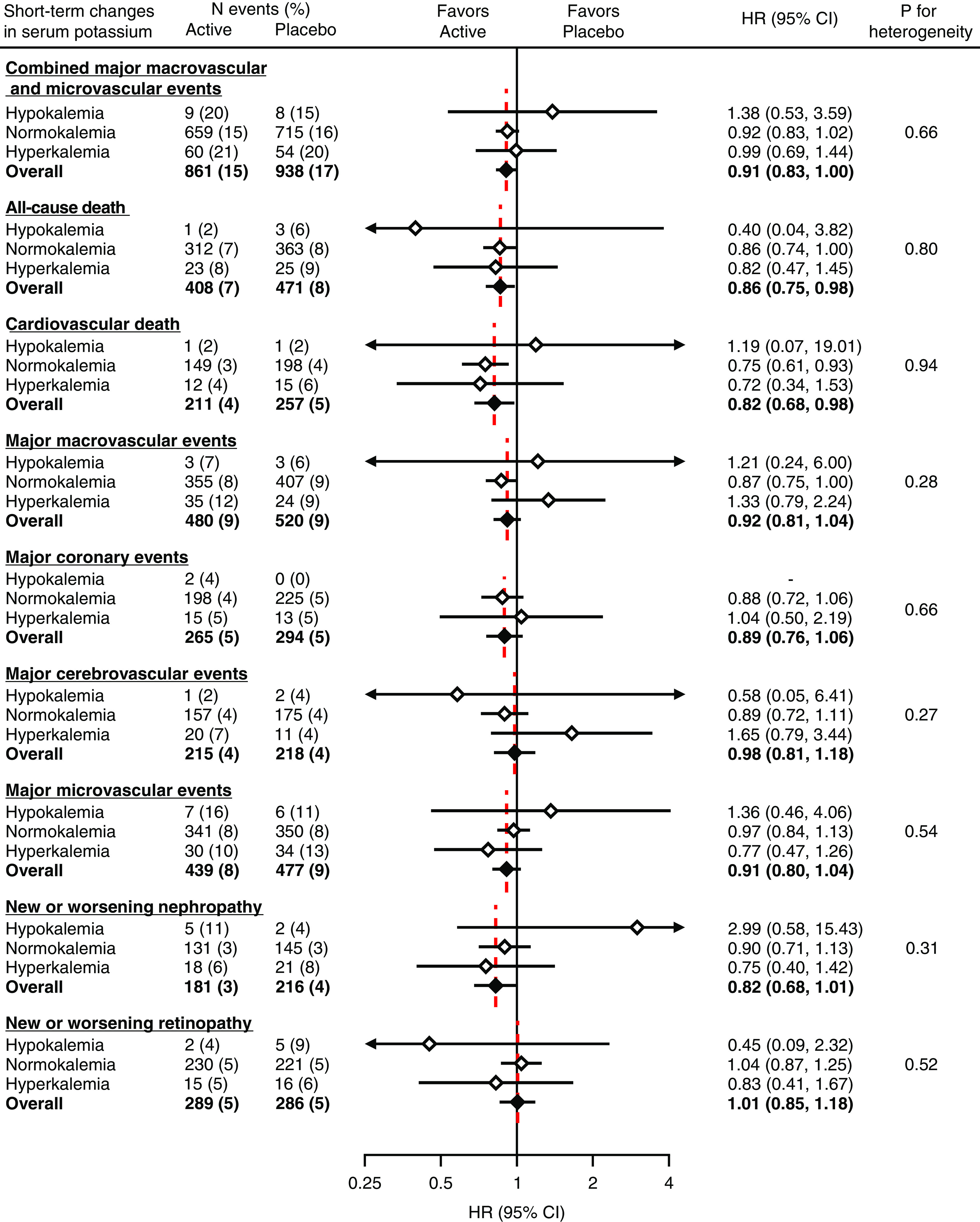
Results: During active run-in, 556 (6%) participants experienced hyperkalemia. During follow-up, 1505 participants experienced the primary composite outcome of major macrovascular and microvascular events. Randomized treatment of angiotensin-converting enzyme inhibitor-based therapy significantly decreased the risk of the primary outcome (38.1 versus 42.0 per 1000 person-years; hazard ratio, 0.91; 95% confidence interval, 0.83 to 1.00; P=0.04) compared with placebo. The magnitude of effects did not differ across subgroups defined by short-term changes in serum potassium during run-in (P for heterogeneity =0.66). Similar consistent treatment effects were also observed for all-cause death, cardiovascular death, major coronary events, major cerebrovascular events, and new or worsening nephropathy (P for heterogeneity ≥0.27).
Conclusions: Continuation of angiotensin-converting enzyme inhibitor-based therapy consistently decreased the subsequent risk of clinical outcomes, including cardiovascular and kidney outcomes and death, regardless of short-term changes in serum potassium.
Clinical trial registry name and registration number: Action in Diabetes and Vascular Disease: Preterax and Diamicron Modified Release Controlled Evaluation (ADVANCE), NCT00145925.
Keywords: ACE inhibitors; discontinuation; hyperkalemia; randomized controlled trials; renin angiotensin system.
Copyright © 2022 by the American Society of Nephrology.
Figures
Comment in
-
Calamari, Hyperkalemia, and Renin-Angiotensin System Blockade.Clin J Am Soc Nephrol. 2022 Aug;17(8):1116-1118. doi: 10.2215/CJN.07280622. Epub 2022 Jul 27. Clin J Am Soc Nephrol. 2022. PMID: 35896278 Free PMC article. No abstract available.
References
-
- Kidney Disease: Improving Global Outcomes Blood Pressure Work Group : KDIGO 2021 clinical practice guideline for the management of blood pressure in chronic kidney disease. Available at: https://kdigo.org/guidelines/blood-pressure-in-ckd/. Accessed June 11, 2022
-
- Ponikowski P, Voors AA, Anker SD, Bueno H, Cleland JGF, Coats AJS, Falk V, González-Juanatey JR, Harjola VP, Jankowska EA, Jessup M, Linde C, Nihoyannopoulos P, Parissis JT, Pieske B, Riley JP, Rosano GMC, Ruilope LM, Ruschitzka F, Rutten FH, van der Meer P; ESC Scientific Document Group : 2016 ESC guidelines for the diagnosis and treatment of acute and chronic heart failure: The Task Force for the diagnosis and treatment of acute and chronic heart failure of the European Society of Cardiology (ESC) developed with the special contribution of the Heart Failure Association (HFA) of the ESC. Eur Heart J 37: 2129–2200, 2016 - PubMed
-
- Yancy CW, Jessup M, Bozkurt B, Butler J, Casey DE Jr., Colvin MM, Drazner MH, Filippatos GS, Fonarow GC, Givertz MM, Hollenberg SM, Lindenfeld J, Masoudi FA, McBride PE, Peterson PN, Stevenson LW, Westlake C: 2017 ACC/AHA/HFSA focused update of the 2013 ACCF/AHA guideline for the management of heart failure: A report of the American College of Cardiology/American Heart Association Task Force on Clinical Practice Guidelines and the Heart Failure Society of America. Circulation 136: e137–e161, 2017 - PubMed
-
- American Diabetes Association : Introduction: Standards of Medical Care in Diabetes-2021. Diabetes Care 44[Suppl 1]: S1–S2, 2021 - PubMed
-
- Cosentino F, Grant PJ, Aboyans V, Bailey CJ, Ceriello A, Delgado V, Federici M, Filippatos G, Grobbee DE, Hansen TB, Huikuri HV, Johansson I, Jüni P, Lettino M, Marx N, Mellbin LG, Östgren CJ, Rocca B, Roffi M, Sattar N, Seferović PM, Sousa-Uva M, Valensi P, Wheeler DC; ESC Scientific Document Group : 2019 ESC guidelines on diabetes, pre-diabetes, and cardiovascular diseases developed in collaboration with the EASD. Eur Heart J 41: 255–323, 2020 - PubMed
Publication types
MeSH terms
Substances
Associated data
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
