

Single-Cell RNA-Seq Identifies Dynamic Cardiac Transition Program from ADCs Induced by Leukemia Inhibitory Factor
- PMID: 35896368
- PMCID: PMC9585902
- DOI: 10.1093/stmcls/sxac048
Single-Cell RNA-Seq Identifies Dynamic Cardiac Transition Program from ADCs Induced by Leukemia Inhibitory Factor
Abstract
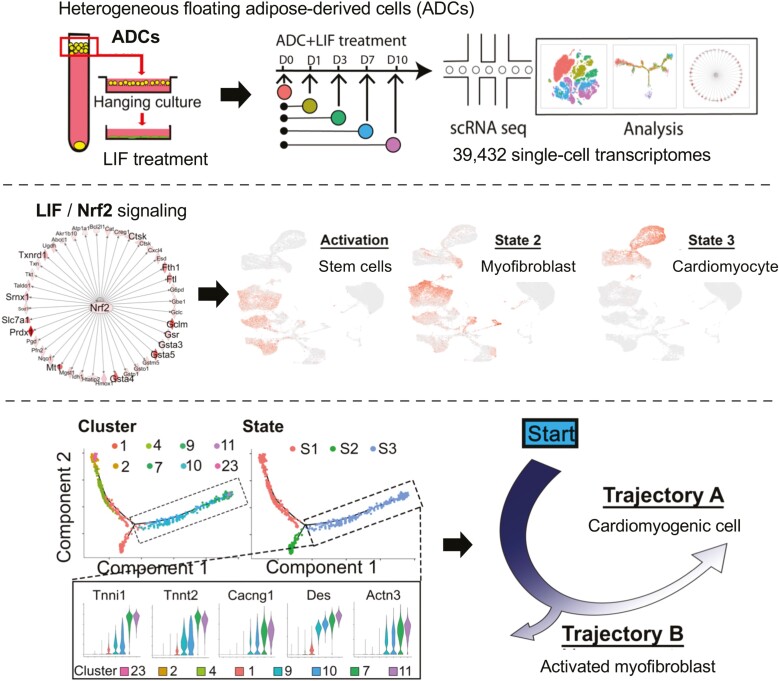
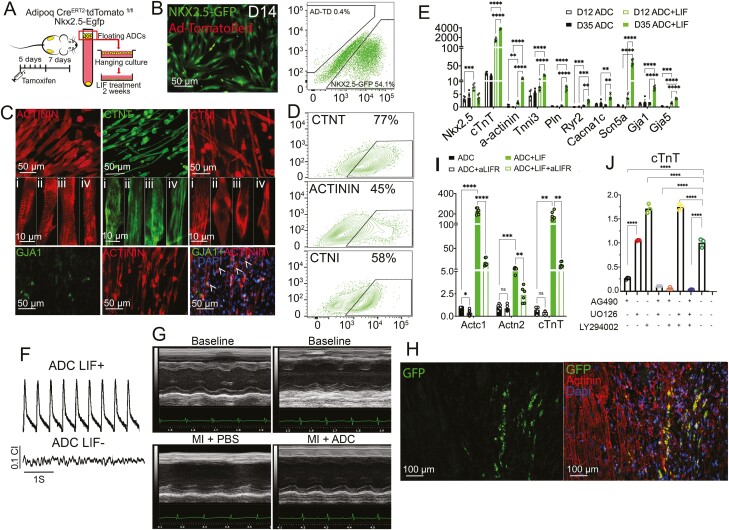
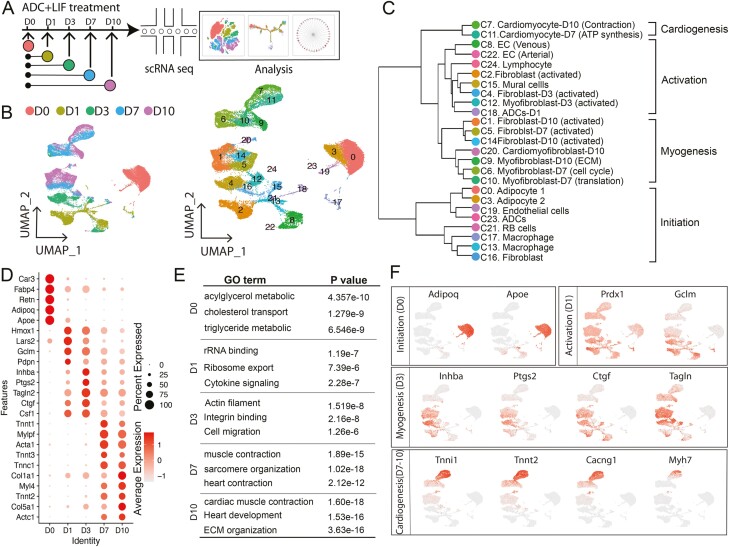
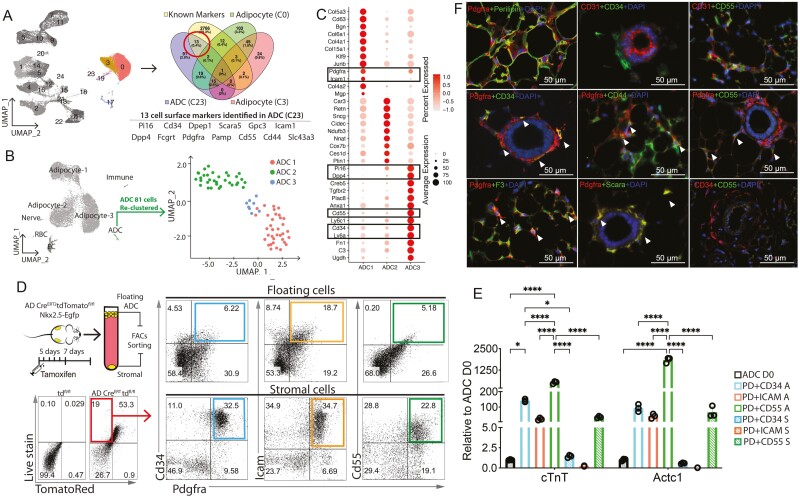
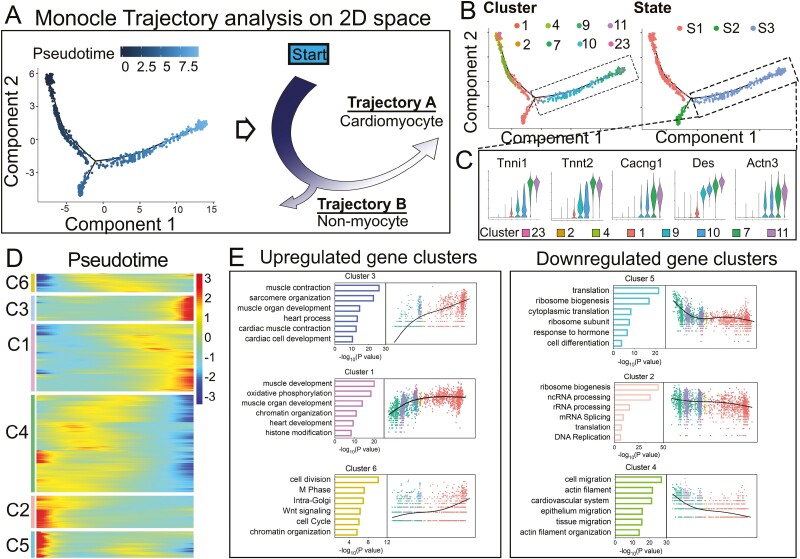
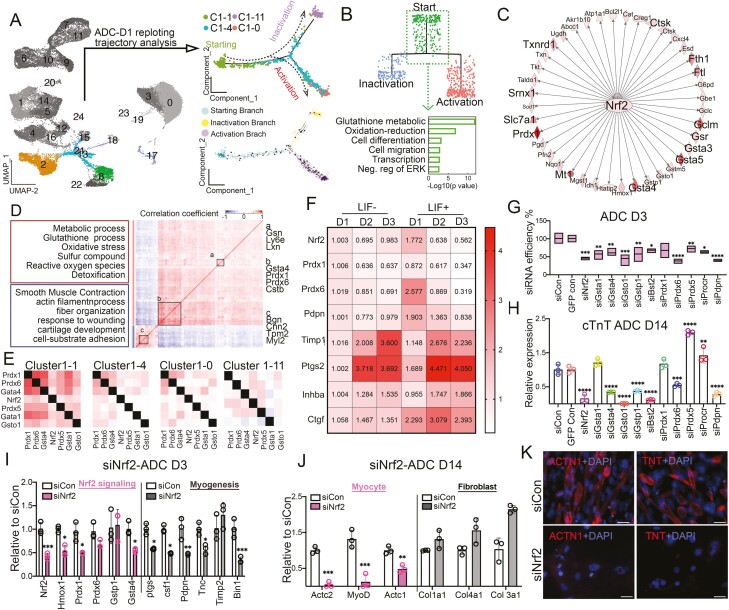
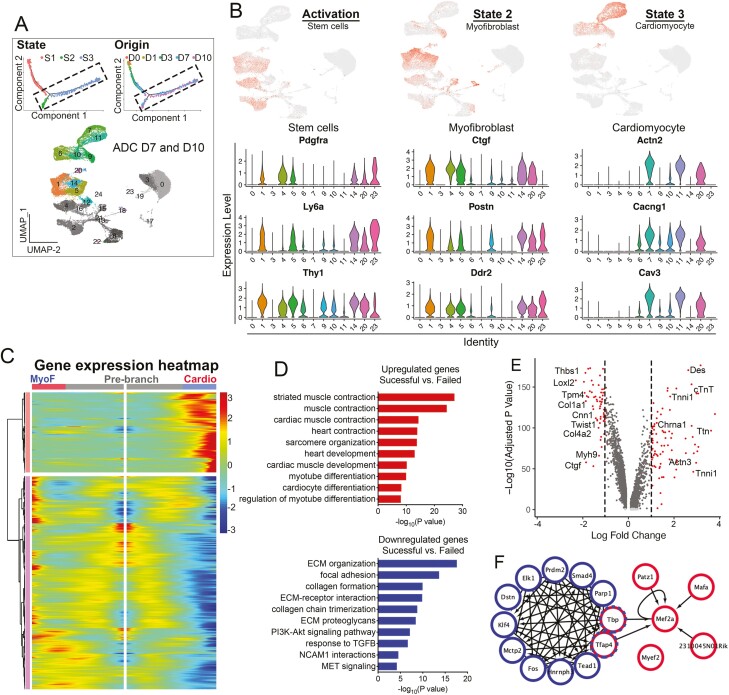
Adipose-derived cells (ADCs) from white adipose tissue are promising stem cell candidates because of their large regenerative reserves and the potential for cardiac regeneration. However, given the heterogeneity of ADC and its unsolved mechanisms of cardiac acquisition, ADC-cardiac transition efficiency remains low. In this study, we explored the heterogeneity of ADCs and the cellular kinetics of 39,432 single-cell transcriptomes along the leukemia inhibitory factor (LIF)-induced ADC-cardiac transition. We identified distinct ADC subpopulations that reacted differentially to LIF when entering the cardiomyogenic program, further demonstrating that ADC-myogenesis is time-dependent and initiates from transient changes in nuclear factor erythroid 2-related factor 2 (Nrf2) signaling. At later stages, pseudotime analysis of ADCs navigated a trajectory with 2 branches corresponding to activated myofibroblast or cardiomyocyte-like cells. Our findings offer a high-resolution dissection of ADC heterogeneity and cell fate during ADC-cardiac transition, thus providing new insights into potential cardiac stem cells.
Keywords: ADC; adipose; cardiac transition; cell sequencing; derived cells; leukemia inhibitory factor (LIF); single.
© The Author(s) 2022. Published by Oxford University Press. All rights reserved. For permissions, please email: journals.permissions@oup.com.
Figures
Similar articles
-
Leukemia Inhibitory Factor Increases Survival of Pluripotent Stem Cell-Derived Cardiomyocytes.J Cardiovasc Transl Res. 2018 Feb;11(1):1-13. doi: 10.1007/s12265-017-9769-6. Epub 2017 Oct 10. J Cardiovasc Transl Res. 2018. PMID: 29019149
-
Leukemia Inhibitory Factor Enhances Endogenous Cardiomyocyte Regeneration after Myocardial Infarction.PLoS One. 2016 May 26;11(5):e0156562. doi: 10.1371/journal.pone.0156562. eCollection 2016. PLoS One. 2016. PMID: 27227407 Free PMC article.
-
STAT3-dependent mouse embryonic stem cell differentiation into cardiomyocytes: analysis of molecular signaling and therapeutic efficacy of cardiomyocyte precommitted mES transplantation in a mouse model of myocardial infarction.Circ Res. 2007 Oct 26;101(9):910-8. doi: 10.1161/CIRCRESAHA.107.156786. Epub 2007 Sep 6. Circ Res. 2007. PMID: 17823373
-
Naive rat amnion-derived cell transplantation improved left ventricular function and reduced myocardial scar of postinfarcted heart.Cell Transplant. 2009;18(4):477-86. doi: 10.3727/096368909788809785. Cell Transplant. 2009. PMID: 19622235
-
LIF and the heart: just another brick in the wall?Eur Cytokine Netw. 2013 Mar;24(1):11-9. doi: 10.1684/ecn.2013.0335. Eur Cytokine Netw. 2013. PMID: 23661360 Free PMC article. Review.
