

Physical and Mental Activity, Disease Susceptibility, and Risk of Dementia: A Prospective Cohort Study Based on UK Biobank
- PMID: 35896434
- PMCID: PMC9484730
- DOI: 10.1212/WNL.0000000000200701
Physical and Mental Activity, Disease Susceptibility, and Risk of Dementia: A Prospective Cohort Study Based on UK Biobank
Abstract
Background and objectives: The association between patterns of physical/mental activity and dementia and how it is affected by disease susceptibility remains unknown. We aimed to examine the association between patterns of physical and mental activity and dementia and whether it can be modified by disease susceptibility to dementia.
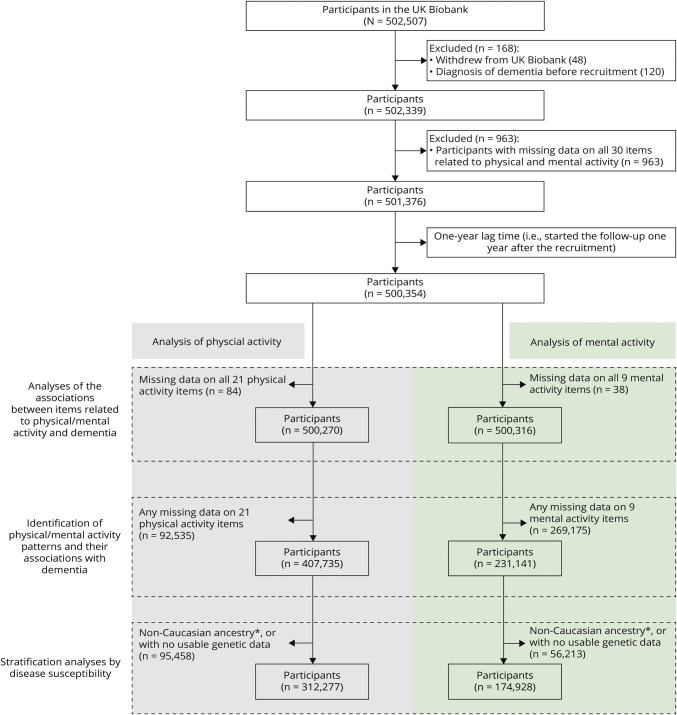
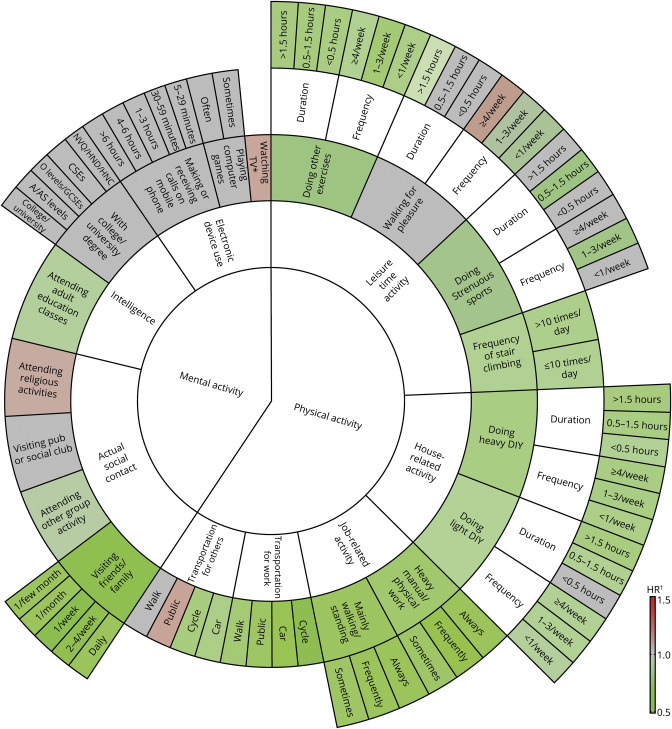
Methods: In a prospective cohort study based on UK Biobank, 501,376 dementia-free participants were recruited in 2006-2010 and followed from 1 year after the recruitment date until the end of 2019 for ascertainment of dementia. Data on physical (i.e., physical activity at leisure time, housework-related activity, and transportation) and mental (i.e., intelligence, social contact, and use of electronic device) activity were collected using questionnaires at recruitment. Cox models were used to estimate the associations of physical and mental activity-related items, as well as major activity patterns identified by principal component analysis, with the risk of dementia, adjusted for multiple confounders. The modification role of disease susceptibility on such associations was assessed through stratified analyses by the polygenic risk score (PRS) of dementia generated based on summary statistics of independent genome-wide association studies, by the APOE genotype, and by the self-reported family history of dementia.
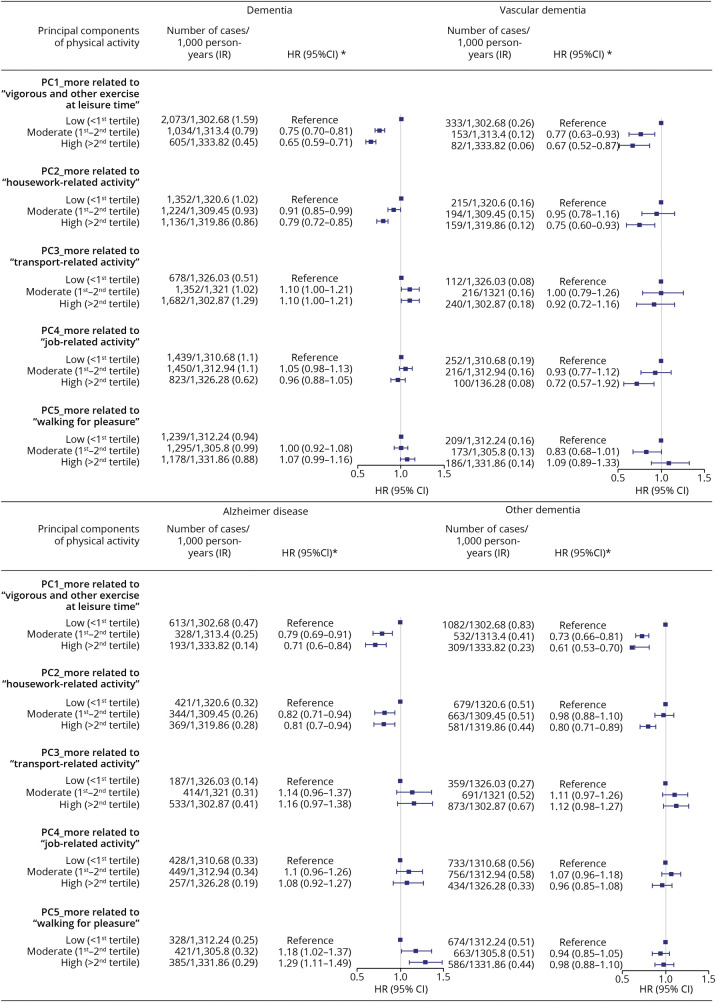
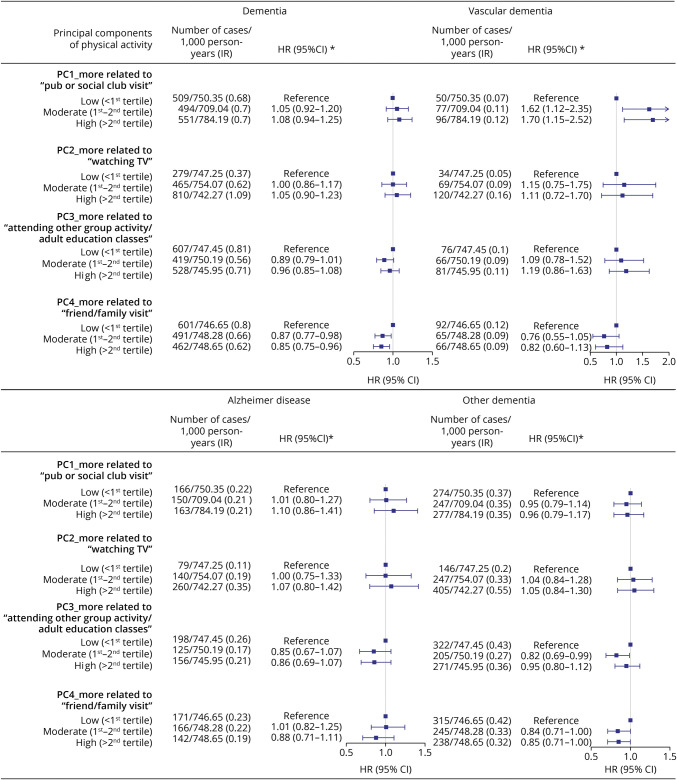
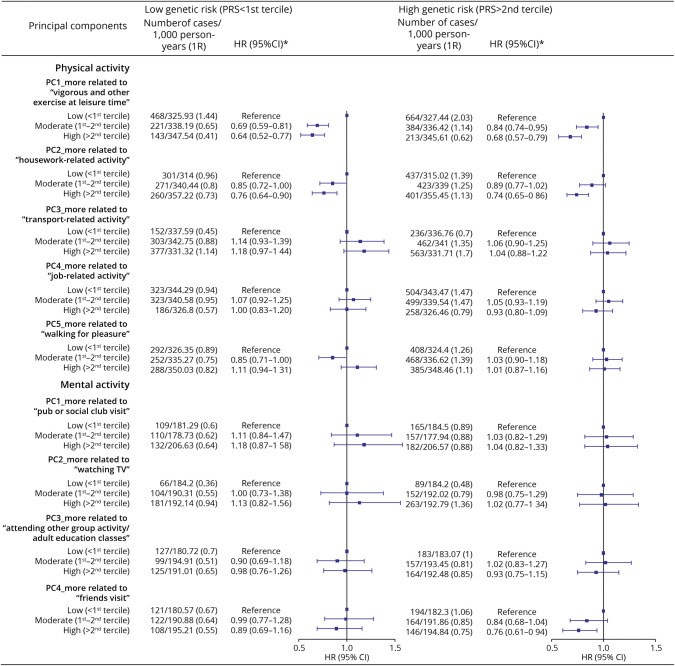
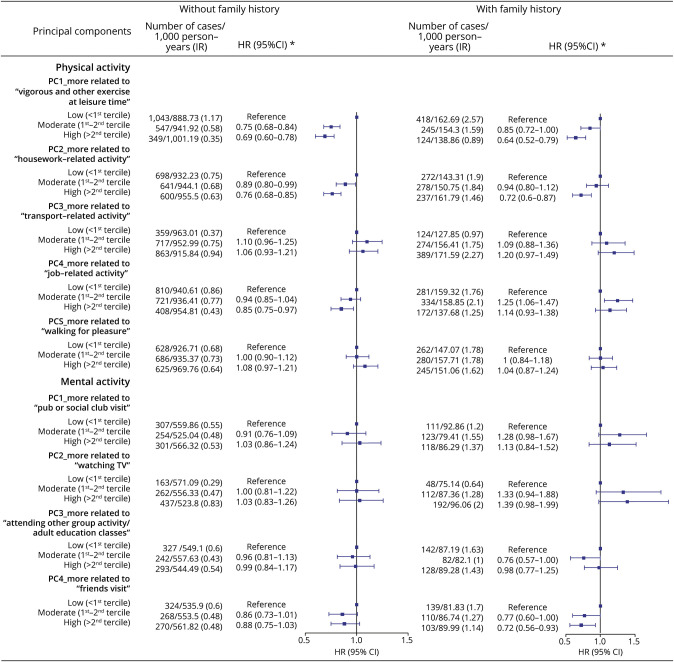
Results: The mean age at recruitment was 56.53, and 45.60% of the participants were male. During a mean follow-up of 10.66 years, 5,185 dementia cases were identified. When analyzed separately, multiple studied items related to physical and mental activity showed significant associations with the risk of dementia. The pattern analyses revealed that a higher level of adherence to activity patterns related to frequent vigorous and other exercises (hazard ratio 0.65, 95% CI 0.59-0.71), housework-related activity (0.79, 0.72-0.85), and friend/family visit (0.85, 0.75-0.96) was associated with a lower risk of dementia. We obtained comparable results for vascular dementia and Alzheimer disease as well as in the stratified analyses by the PRS for dementia, APOE genotype, or family history of dementia.
Discussion: Activity patterns more adherent to frequent vigorous and other exercises, housework-related activity, and friend/family visit were associated with a reduced risk of multiple types of dementia. Such associations are independent of disease susceptibility, highlighting the potential of these physical and mental activity patterns, as effective interventions, in the primary prevention of dementia.
Copyright © 2022 The Author(s). Published by Wolters Kluwer Health, Inc. on behalf of the American Academy of Neurology.
Figures
References
-
- Angevaren M, Aufdemkampe G, Verhaar HJ, Aleman A, Vanhees L. Physical activity and enhanced fitness to improve cognitive function in older people without known cognitive impairment. Cochrane Database Syst Rev. 2008(3):Cd005381. - PubMed
-
- Walsh EI, Smith L, Northey J, Rattray B, Cherbuin N. Towards an understanding of the physical activity-BDNF-cognition triumvirate: a review of associations and dosage. Ageing Res Rev. 2020;60:101044. - PubMed
-
- Livingston G, Sommerlad A, Orgeta V, et al. Dementia prevention, intervention, and care. Lancet. 2017;390(10113):2673-2734. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Miscellaneous