

The Effect of Digitization on the Safe Management of Anticoagulants
- PMID: 35896507
- PMCID: PMC9474267
- DOI: 10.1055/a-1910-4339
The Effect of Digitization on the Safe Management of Anticoagulants
Abstract
Background: Anticoagulants are high-risk medications and are a common cause of adverse events of hospitalized inpatients. The incidence of adverse events involving anticoagulants has remained relatively unchanged over the past two decades, suggesting that novel approaches are required to address this persistent issue. Electronic medication management systems (eMMSs) offer strategies to help reduce medication incidents and adverse drug events, yet poor system design can introduce new error types.
Objective: Our objective was to evaluate the effect of the introduction of an electronic medical record (EMR) on the quality and safety of therapeutic anticoagulation management.
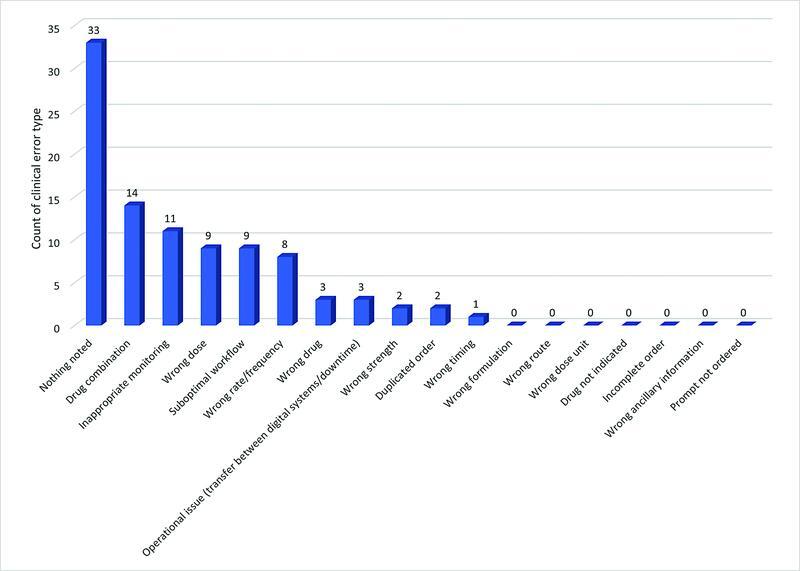
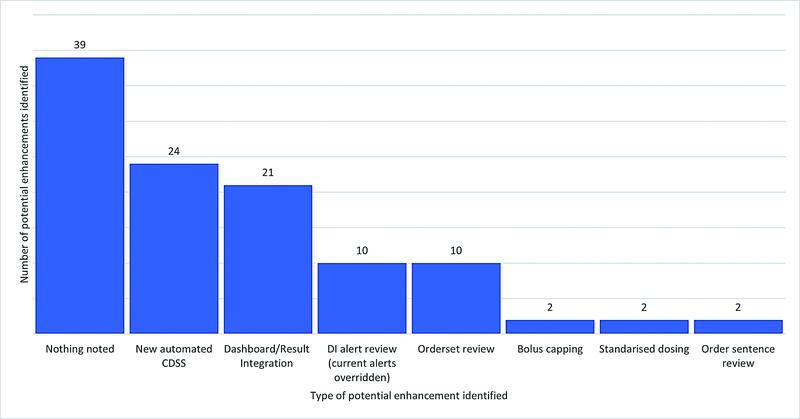
Methods: A retrospective, observational pre-/poststudy was conducted, analyzing real-world data across five hospital sites in a single health service. Four metrics were compared 1-year pre- and 1-year post-EMR implementation. They included clinician-reported medication incidents, toxic pathology results, hospital-acquired bleeding complications (HACs), and rate of heparin-induced thrombocytopenia. Further subanalyses of patients experiencing HACs in the post-EMR period identified key opportunities for intervention to maximize safety and quality of anticoagulation within an eMMS.
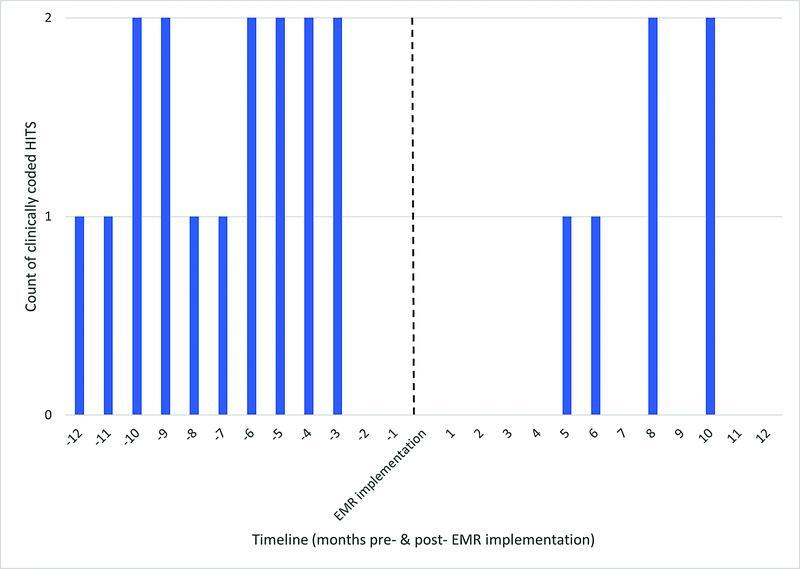
Results: A significant reduction in HACs was observed in the post-EMR implementation period (mean [standard deviation [SD]] =12.1 [4.4]/month vs. mean [SD] = 7.8 [3.5]/month; p = 0.01). The categorization of potential EMR design enhancements found that new automated clinical decision support or improved pathology result integration would be suitable to mitigate future HACs in an eMMS. There was no significant difference in the mean monthly clinician-reported incident rates for anticoagulants or the rate of toxic pathology results in the pre- versus post-EMR implementation period. A 62.5% reduction in the cases of heparin-induced thrombocytopenia was observed in the post-EMR implementation period.
Conclusion: The implementation of an EMR improves clinical care outcomes for patients receiving anticoagulation. System design plays a significant role in mitigating the risks associated with anticoagulants and consideration must be given to optimizing eMMSs.
The Author(s). This is an open access article published by Thieme under the terms of the Creative Commons Attribution License, permitting unrestricted use, distribution, and reproduction so long as the original work is properly cited. (https://creativecommons.org/licenses/by/4.0/).
Conflict of interest statement
None declared.
Figures
References
-
- Australasian Society of Thrombosis and Haemostasis . Tran H, Joseph J, Young L. New oral anticoagulants: a practical guide on prescription, laboratory testing and peri-procedural/bleeding management. Intern Med J. 2014;44(06):525–536. - PubMed
-
- Australasian Society of Thrombosis and Haemostasis (ASTH) . Tran H A, Chunilal S D, Harper P L, Tran H, Wood E M, Gallus A S. An update of consensus guidelines for warfarin reversal. Med J Aust. 2013;198(04):198–199. - PubMed
-
- Zimmermann A T, Jeffries W S, McElroy H, Horowitz J D.Utility of a weight-based heparin nomogram for patients with acute coronary syndromes Intern Med J 200333(1-2):18–25. - PubMed
-
- Australian Commission on Safety and Quality in Health Care High risk medicines 2018 [cited 2022, 26 Feb]Accessed August 08, 2022 at:https://www.safetyandquality.gov.au/our-work/medication-safety/high-risk...
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Miscellaneous