

Determination of significant parameters in remote ischemic postconditioning for ischemic stroke in experimental models: A systematic review and meta-analysis study
- PMID: 35896511
- PMCID: PMC9437239
- DOI: 10.1111/cns.13925
Determination of significant parameters in remote ischemic postconditioning for ischemic stroke in experimental models: A systematic review and meta-analysis study
Abstract
Objectives: To systematically review studies using remote ischemia postconditioning (RIPostC) for ischemic stroke in experimental models and obtain factors that significantly influence treatment outcomes.
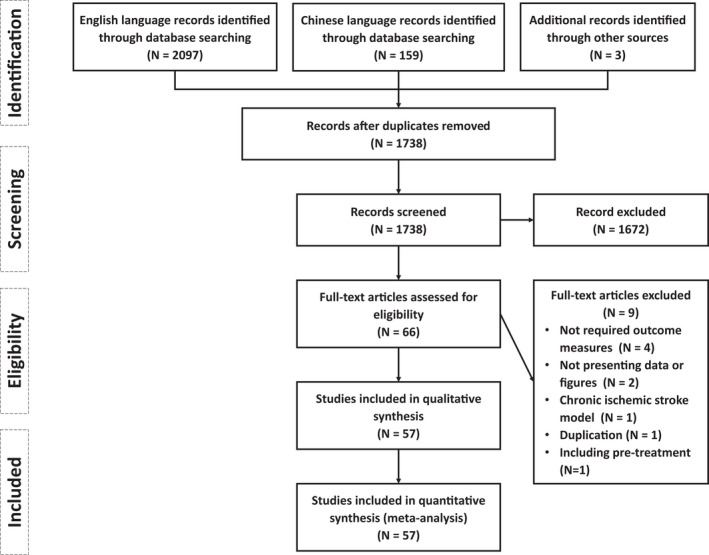
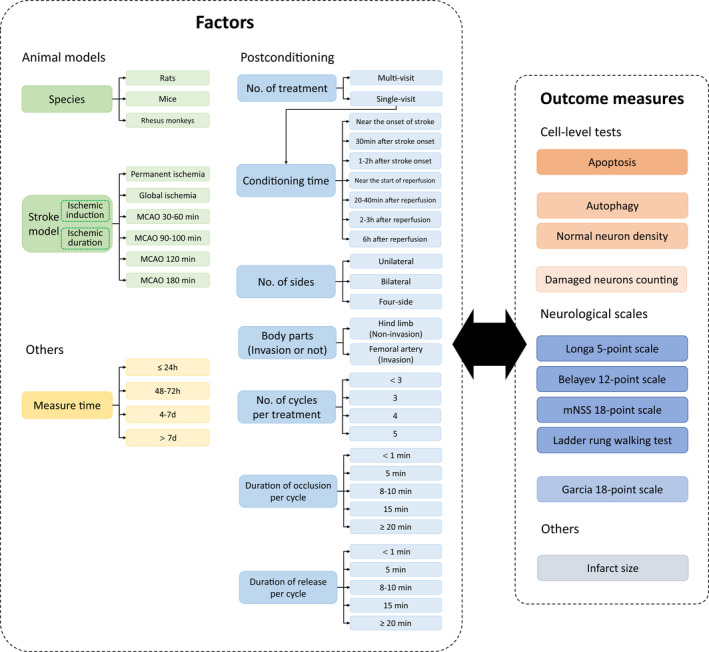
Materials and methods: Peer-reviewed studies were identified and selected based on the eligibility criteria, followed by extraction of data on potentially influential factors related to model preparation, postconditioning, and measure time based on outcome measures including infarct size, neurological scales, and cell tests with autophagy, apoptosis, normal-neuron, and damaged-neuron counting. Then, all data were preprocessed, grouped, and meta-analyzed with the indicator of the standardized mean difference.
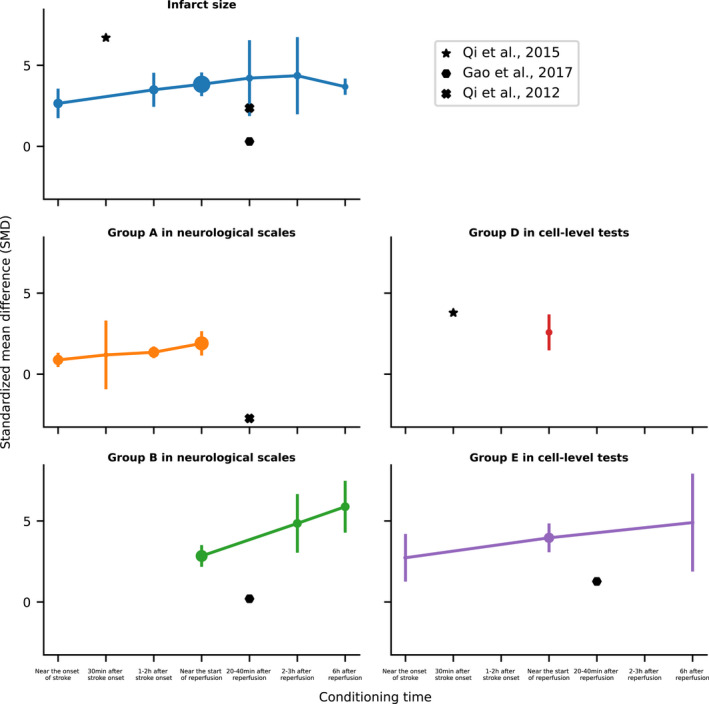
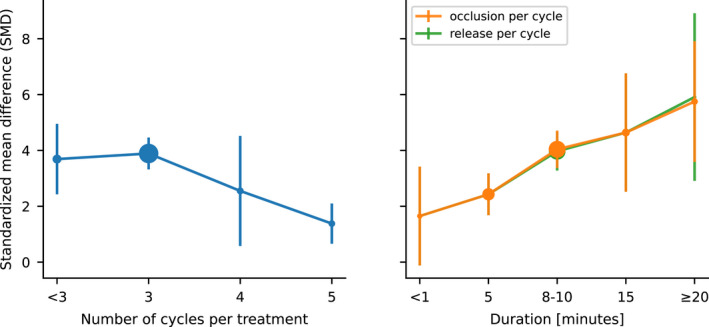
Results: Fifty-seven studies with 224 experiments (91 for infarct size, 92 for neurological scales, and 41 for cell-level tests) were included. There was little statistical difference between different model preparations, treated body parts, number of treatments, and sides. And treatment effect was generally a positive correlation with the duration of conditioning time to stroke onset with exceptions at some time points. Based on infarct size, the number of cycles per treatment, duration of occlusion, and release per cycle showed significant differences. Combined with the effect sizes by other measures, the occlusion/release duration of 8-10 min per cycle is better than 5 min, and three cycles per treatment were most frequently used with good effects. Effect also varied when measuring at different times, showing statistical differences in infarct size and most neurological scales. RIPostC is confirmed as an effective therapeutic intervention for ischemic stroke, while the RIPostC-mediated autophagy level being activated or inhibited remained conflicting.
Conclusions: Conditioning time, number of cycles per treatment, duration of occlusion, and release per cycle were found to influence the treatment effects of RIPostC significantly. More studies on the relevant influential factors and autophagy mechanisms are warranted.
Keywords: experimental models; ischemia; meta-analysis; remote ischemic postconditioning; stroke.
© 2022 The Authors. CNS Neuroscience & Therapeutics published by John Wiley & Sons Ltd.
Conflict of interest statement
The authors declare no conflicts of interest. The authors alone are responsible for the contents and writing of the article.
Figures
Similar articles
-
Adefovir dipivoxil and pegylated interferon alfa-2a for the treatment of chronic hepatitis B: a systematic review and economic evaluation.Health Technol Assess. 2006 Aug;10(28):iii-iv, xi-xiv, 1-183. doi: 10.3310/hta10280. Health Technol Assess. 2006. PMID: 16904047
-
Home treatment for mental health problems: a systematic review.Health Technol Assess. 2001;5(15):1-139. doi: 10.3310/hta5150. Health Technol Assess. 2001. PMID: 11532236
-
Remote Ischemic Postconditioning Improve Cerebral Ischemia-Reperfusion Injury Induced Cognitive Dysfunction through Suppressing Mitochondrial Apoptosis in Hippocampus via TK/BK/B2R-Mediated PI3K/AKT.Mol Neurobiol. 2025 Aug;62(8):10652-10669. doi: 10.1007/s12035-025-04864-y. Epub 2025 Apr 14. Mol Neurobiol. 2025. PMID: 40229456 Free PMC article.
-
A rapid and systematic review of the clinical effectiveness and cost-effectiveness of paclitaxel, docetaxel, gemcitabine and vinorelbine in non-small-cell lung cancer.Health Technol Assess. 2001;5(32):1-195. doi: 10.3310/hta5320. Health Technol Assess. 2001. PMID: 12065068
-
A rapid and systematic review of the clinical effectiveness and cost-effectiveness of topotecan for ovarian cancer.Health Technol Assess. 2001;5(28):1-110. doi: 10.3310/hta5280. Health Technol Assess. 2001. PMID: 11701100
Cited by
-
Targeting cell death pathways in intestinal ischemia-reperfusion injury: a comprehensive review.Cell Death Discov. 2024 Mar 4;10(1):112. doi: 10.1038/s41420-024-01891-x. Cell Death Discov. 2024. PMID: 38438362 Free PMC article. Review.
-
Efficacy and safety of remote ischemic conditioning for acute ischemic stroke: A comprehensive meta-analysis from randomized controlled trials.CNS Neurosci Ther. 2023 Sep;29(9):2445-2456. doi: 10.1111/cns.14240. Epub 2023 May 14. CNS Neurosci Ther. 2023. PMID: 37183341 Free PMC article. Review.
-
Impact of remote ischemic postconditioning on acute ischemic stroke in China: a systematic review and meta-analysis of randomized controlled trials.Syst Rev. 2024 May 30;13(1):141. doi: 10.1186/s13643-024-02568-3. Syst Rev. 2024. PMID: 38816852 Free PMC article.
-
The potential mechanism and clinical application value of remote ischemic conditioning in stroke.Neural Regen Res. 2025 Jun 1;20(6):1613-1627. doi: 10.4103/NRR.NRR-D-23-01800. Epub 2024 Jun 3. Neural Regen Res. 2025. PMID: 38845225 Free PMC article.
-
Clemastine Reduces post-stroke Neurodegeneration by Alleviating Endoplasmic Reticulum stress-mediated Demyelination and Cognitive Impairment Through PERK/ATF4/CHOP Signaling Pathway.Neurochem Res. 2025 Apr 25;50(3):151. doi: 10.1007/s11064-025-04403-0. Neurochem Res. 2025. PMID: 40274676
References
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
