

Diffuse correlation spectroscopy blood flow monitoring for intraventricular hemorrhage vulnerability in extremely low gestational age newborns
- PMID: 35896691
- PMCID: PMC9329437
- DOI: 10.1038/s41598-022-16499-3
Diffuse correlation spectroscopy blood flow monitoring for intraventricular hemorrhage vulnerability in extremely low gestational age newborns
Abstract
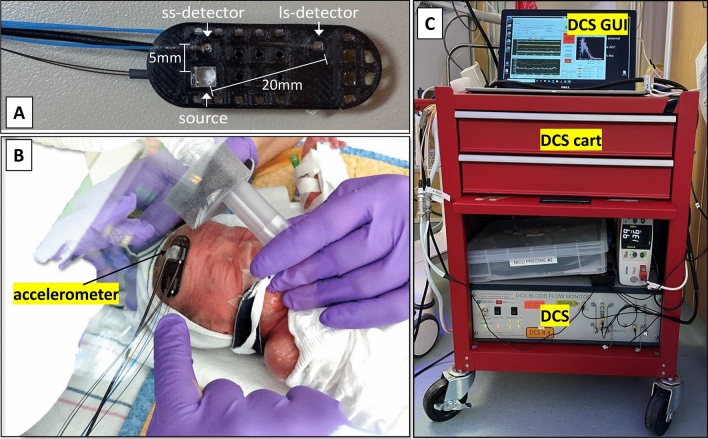
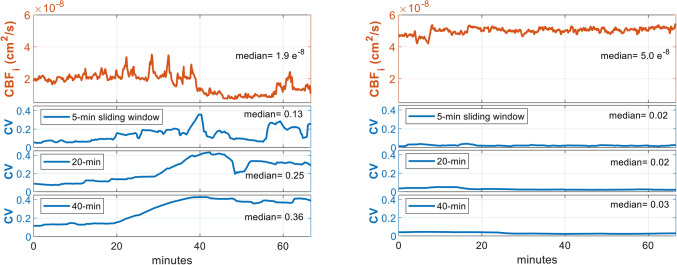
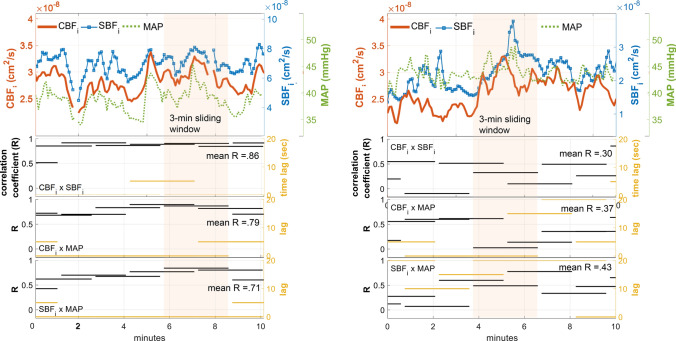
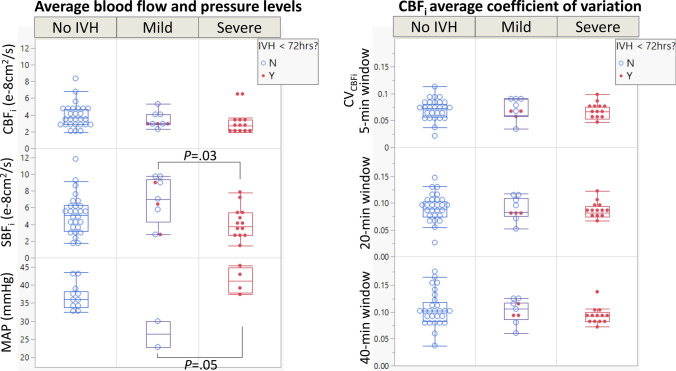
In premature infants with an extremely low gestational age (ELGA, < 29 weeks GA), dysregulated changes in cerebral blood flow (CBF) are among the major pathogenic factors leading to germinal matrix/intraventricular hemorrhage (GM/IVH). Continuous monitoring of CBF can guide interventions to minimize the risk of brain injury, but there are no clinically standard techniques or tools for its measurement. We report the feasibility of the continuous monitoring of CBF, including measures of autoregulation, via diffuse correlation spectroscopy (DCS) in ELGA infants using CBF variability and correlation with scalp blood flow (SBF, served as a surrogate measure of systemic perturbations). In nineteen ELGA infants (with 9 cases of GM/IVH) monitored for 6-24 h between days 2-5 of life, we found a strong correlation between CBF and SBF in severe IVH (Grade III or IV) and IVH diagnosed within 72 h of life, while CBF variability alone was not associated with IVH. The proposed method is potentially useful at the bedside for the prompt assessment of cerebral autoregulation and early identification of infants vulnerable to GM/IVH.
© 2022. The Author(s).
Conflict of interest statement
The authors, except MAF, declare no conflicts of interest in this work. MAF has a financial interest in 149 Medical, Inc., a company developing DCS technology for assessing and monitoring cerebral blood flow in newborn infants. MAF’s interests were reviewed and are managed by Massachusetts General Hospital and Mass General Brigham in accordance with their conflict of interest policies.
Figures
References
-
- Horbar JD. Vermont Oxford Network Database Summary for Infants 501 to 1500 Grams Born in 2020. Springer; 2020.
-
- Walsh, B. H., Inder, T. E. & Volpe, J. J. Intraventricular hemorrhage in the neonate. in Fetal and Neonatal Physiology 1333–1349 (Elsevier, 2017). 10.1016/B978-0-323-35214-7.00134-7.
-
- Murphy SL, Mathews TJ, Martin JA, Minkovitz CS, Strobino DM. Annual summary of vital statistics: 2013–2014. Pediatrics. 2017;139:2013–2014. - PubMed
-
- Inder TE, Perlman JM, Volpe JJ. Preterm Intraventricular Hemorrhage/Posthemorrhagic Hydrocephalus. Volpe’s Neurology of the Newborn. Elsevier Inc; 2017.
-
- Perlman JM, Volpe JJ. Intraventricular hemorrhage in extremely small premature infants. Am. J. Dis. Child. 1986;140:1122–1124. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
