

Cardiac Arrest Treatment Center Differences in Sedation and Analgesia Dosing During Targeted Temperature Management
- PMID: 35896768
- PMCID: PMC9935704
- DOI: 10.1007/s12028-022-01564-6
Cardiac Arrest Treatment Center Differences in Sedation and Analgesia Dosing During Targeted Temperature Management
Abstract
Background: Sedation and analgesia are recommended during targeted temperature management (TTM) after cardiac arrest, but there are few data to provide guidance on dosing to bedside clinicians. We evaluated differences in patient-level sedation and analgesia dosing in an international multicenter TTM trial to better characterize current practice and clinically important outcomes.
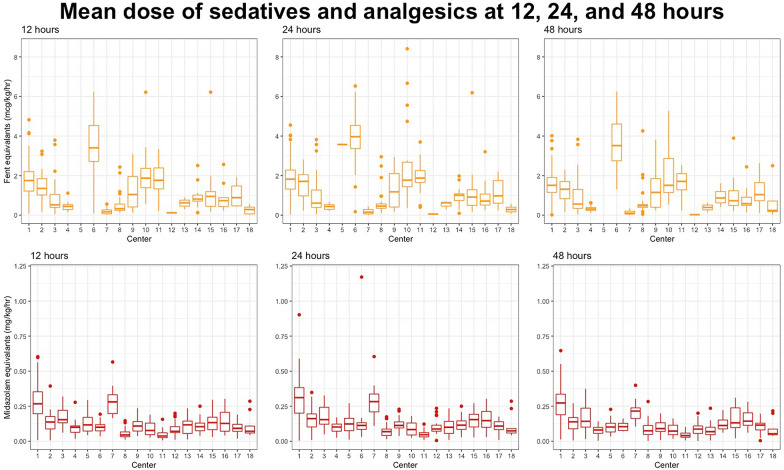
Methods: A total 950 patients in the international TTM trial were randomly assigned to a TTM of 33 °C or 36 °C after resuscitation from cardiac arrest in 36 intensive care units. We recorded cumulative doses of sedative and analgesic drugs at 12, 24, and 48 h and normalized to midazolam and fentanyl equivalents. We compared number of medications used, dosing, and titration among centers by using multivariable models, including common severity of illness factors. We also compared dosing with time to awakening, incidence of clinical seizures, and survival.
Results: A total of 614 patients at 18 centers were analyzed. Propofol (70%) and fentanyl (51%) were most frequently used. The average dosages of midazolam and fentanyl equivalents were 0.13 (0.07, 0.22) mg/kg/h and 1.16 (0.49, 1.81) µg/kg/h, respectively. There were significant differences in number of medications (p < 0.001), average dosages (p < 0.001), and titration at all time points between centers (p < 0.001), and the outcomes of patients in these centers were associated with all parameters described in the multivariate analysis, except for a difference in the titration of sedatives between 12 and 24 h (p = 0.40). There were associations between higher dosing at 48 h (p = 0.003, odds ratio [OR] 1.75) and increased titration of analgesics between 24 and 48 h (p = 0.005, OR 4.89) with awakening after 5 days, increased titration of sedatives between 24 and 48 h with awakening after 5 days (p < 0.001, OR > 100), and increased titration of sedatives between 24 and 48 h with a higher incidence of clinical seizures in the multivariate analysis (p = 0.04, OR 240). There were also significant associations between decreased titration of analgesics and survival at 6 months in the multivariate analysis (p = 0.048).
Conclusions: There is significant variation in choice of drug, dosing, and titration when providing sedation and analgesics between centers. Sedation and analgesia dosing and titration were associated with delayed awakening, incidence of clinical seizures, and survival, but the causal relation of these findings cannot be proven.
Keywords: Analgesia; Analgosedation; Cardiac arrest; Sedation; Seizures; Target temperature management.
© 2022. The Author(s).
Conflict of interest statement
The authors declare that they have no conflicts of interest.
Figures
References
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
