

Trans-sacral screw fixation of posterior pelvic ring injuries: review and expert opinion
- PMID: 35897108
- PMCID: PMC9327417
- DOI: 10.1186/s13037-022-00333-w
Trans-sacral screw fixation of posterior pelvic ring injuries: review and expert opinion
Abstract
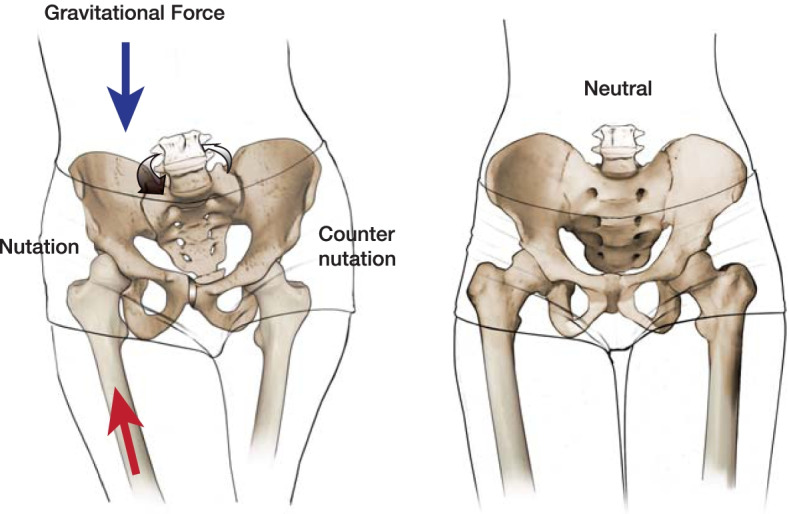
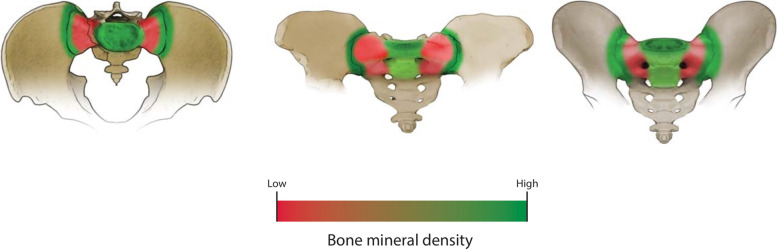
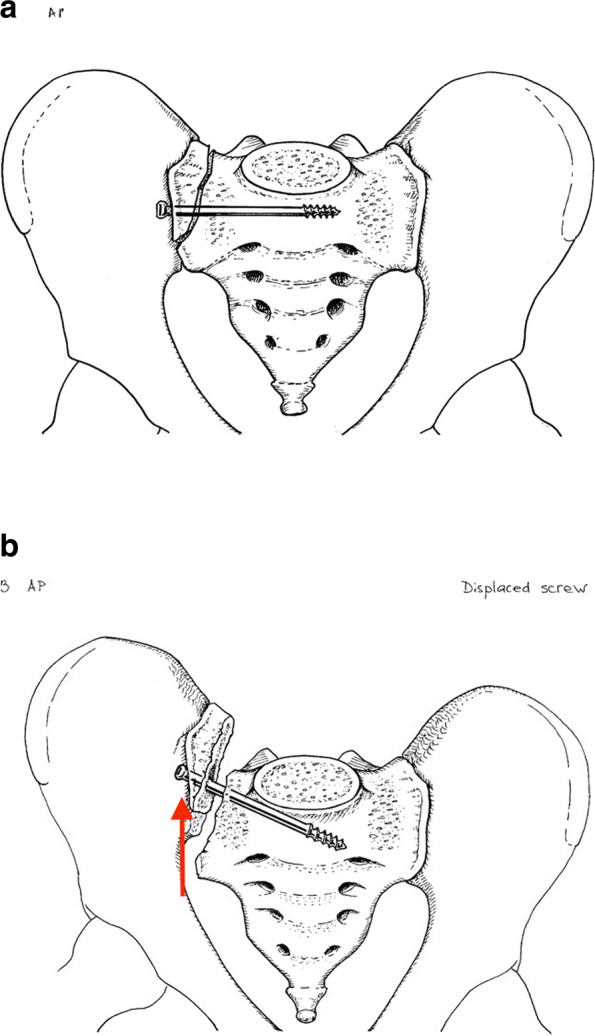
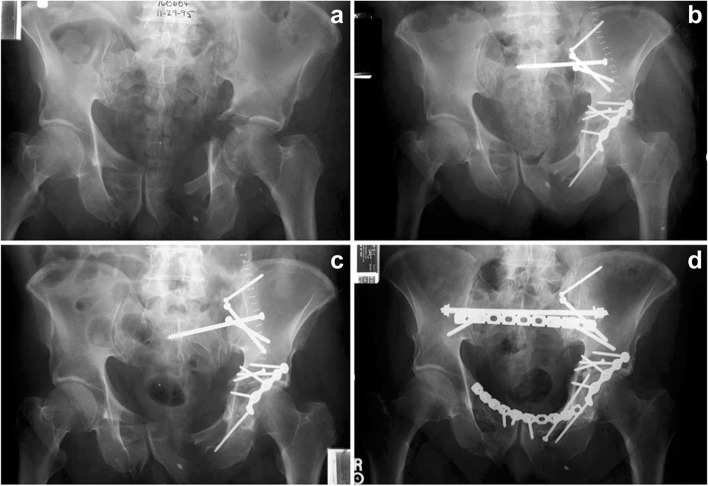
Posterior pelvic ring injuries (i.e., sacro-iliac joint dislocations, fracture-dislocations, sacral fractures, pelvic non-unions/malunions) are challenging injury patterns which require a significant level of surgical training and technical expertise. The modality of surgical management depends on the specific injury patterns, including the specific bony fracture pattern, ilio-sacral joint involvement, and the soft tissue injury pattern. The workhorse for posterior pelvic ring stabilization has been cannulated iliosacral screws, however, trans-sacral screws may impart increased fixation strength. Depending on injury pattern and sacral anatomy, trans-sacral screws can potentially be more beneficial than iliosacral screws. In this article, the authors will briefly review pelvic mechanics and discuss their rationale for ilio-sacral and/or trans-sacral screw fixation.
Keywords: Iliosacral; Injury mechanism; Pelvic fracture; Posterior pelvic ring; Screw; Trans-sacral.
© 2022. The Author(s).
Conflict of interest statement
The authors declare that they have no competing interests.
Figures

References
-
- Ziran NM, Smith WR. Pelvic fractures. Management of musculoskeletal injuries in the trauma patient. New York: Springer; 2014. pp. 143–163.
-
- Tile M, Helfet D. Fractures of the pelvis and acetabulum. 3. Baltimore: Williams & Wilkins; 2003.
-
- Gray’s Anatomy. The anatomical basis of clinical practice. 41st ed. Standring S editor. New York: Elsevier Limited; 2016.
-
- Chamberlain WE. The symphysis pubis in the roentgen examination of the sacro-iliac joint. Am J Roentgenol. 1930;24:621–625.
-
- Chamberlain WE. The X-ray examination of the sacroiliac joint. Delaware Med J. 1932;4:195–201.
Publication types
LinkOut - more resources
Full Text Sources
