

The progression-free survival ratio as outcome measure in recurrent ovarian carcinoma patients: Current and future perspectives
- PMID: 35898197
- PMCID: PMC9309411
- DOI: 10.1016/j.gore.2022.101035
The progression-free survival ratio as outcome measure in recurrent ovarian carcinoma patients: Current and future perspectives
Abstract
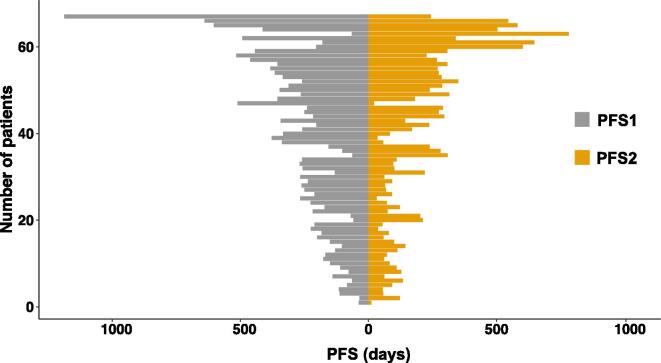
Objective: Clinical efficacy of cytostatic anticancer agents can be determined with the progression-free survival (PFS) ratio. This outcome measure compares PFS achieved by a new treatment (PFS2) to the PFS of the most recent treatment on which the patient has experienced progression (PFS1). Clinical benefit has been defined as a PFS-ratio (PFS2/PFS1) > 1.3. However, in order to demonstrate significant benefit, trial designs require an assumption on the proportion of patients who reach this ratio during palliative options. For ovarian carcinoma, data is lacking to support this assumption. Therefore in this study, we assess the PFS-ratio in recurrent ovarian carcinoma patients treated with current palliative options.
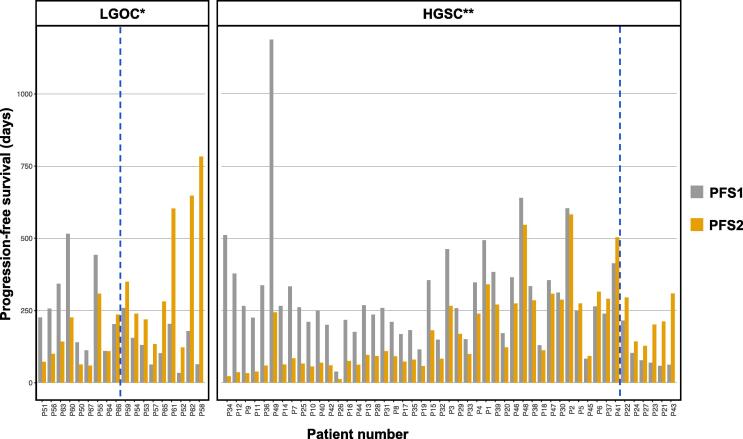
Methods: We included 67 patients with recurrent high-grade serous (HGSC, 73.1%) or low-grade (LGOC, 26.9%) ovarian carcinoma. We determined the median PFS-ratio and investigated the association with clinicopathological characteristics.
Results: Overall, we observed a median PFS-ratio of 0.69. The proportion of patients with a PFS-ratio > 1.3 was 22.4%. For HGSC patients, the median PFS-ratio was significantly lower than for LGOC patients (respectively, 0.58 and 1.26, p = 0.007). Multivariate logistic regression analysis revealed that the LGOC subtype and CA125 tumor marker concentration were independent factors related to a PFS-ratio > 1.3.
Conclusions: Although the PFS-ratio represents a meaningful outcome measure in studies investigating cytostatic anticancer agents, we conclude that it is influenced by tumor histology and biological behavior. In future research, these factors should be taken into account when determining thresholds for clinical benefit in trial designs.
Keywords: Growth-modulation index; Ovarian cancer; Ovarian carcinoma; Progression-free survival ratio; Time to progression ratio.
© 2022 Published by Elsevier Inc.
Conflict of interest statement
The authors declare that they have no known competing financial interests or personal relationships that could have appeared to influence the work reported in this paper.
Figures
References
-
- von Hoff D. There are no bad anticancer agents, only bad clinical trial designs–twenty-first Richard and Hinda Rosenthal Foundation Award Lecture. Clin Cancer Res. 1998;4:1079–1086. - PubMed
-
- Von Hoff D.D., Stephenson J.J., Rosen P., Loesch D.M., Borad M.J., Anthony S., Jameson G., Brown S., Cantafio N., Richards D.A., Fitch T.R., Wasserman E., Fernandez C., Green S., Sutherland W., Bittner M., Alarcon A., Mallery D., Penny R. Pilot Study Using Molecular Profiling of Patients’ Tumors to Find Potential Targets and Select Treatments for Their Refractory Cancers. J. Clin. Oncol. 2010;28(33):4877–4883. - PubMed
LinkOut - more resources
Full Text Sources
Research Materials
Miscellaneous