

Risk factors, mortality trends and cardiovasuclar diseases in people with Type 1 diabetes and controls: A Swedish observational cohort study
- PMID: 35898332
- PMCID: PMC9309414
- DOI: 10.1016/j.lanepe.2022.100469
Risk factors, mortality trends and cardiovasuclar diseases in people with Type 1 diabetes and controls: A Swedish observational cohort study
Abstract
Background: Historically, the incidence of cardiovascular disease and mortality in persons with Type 1 diabetes (T1D) has been increased compared to the general population. Contemporary studies on time trends of mortality and cardiovascular disease are sparse.
Methods: In this observational study, T1D persons were identified in the Swedish National Diabetes Registry (n=45,575) and compared with matched controls from the general population (n=220,141). Incidence rates from 2002 to 2019 were estimated with respect to mortality and cardiovascular disease in persons with T1D overall and when stratified for prevalent cardiovascular and renal disease relative to controls.
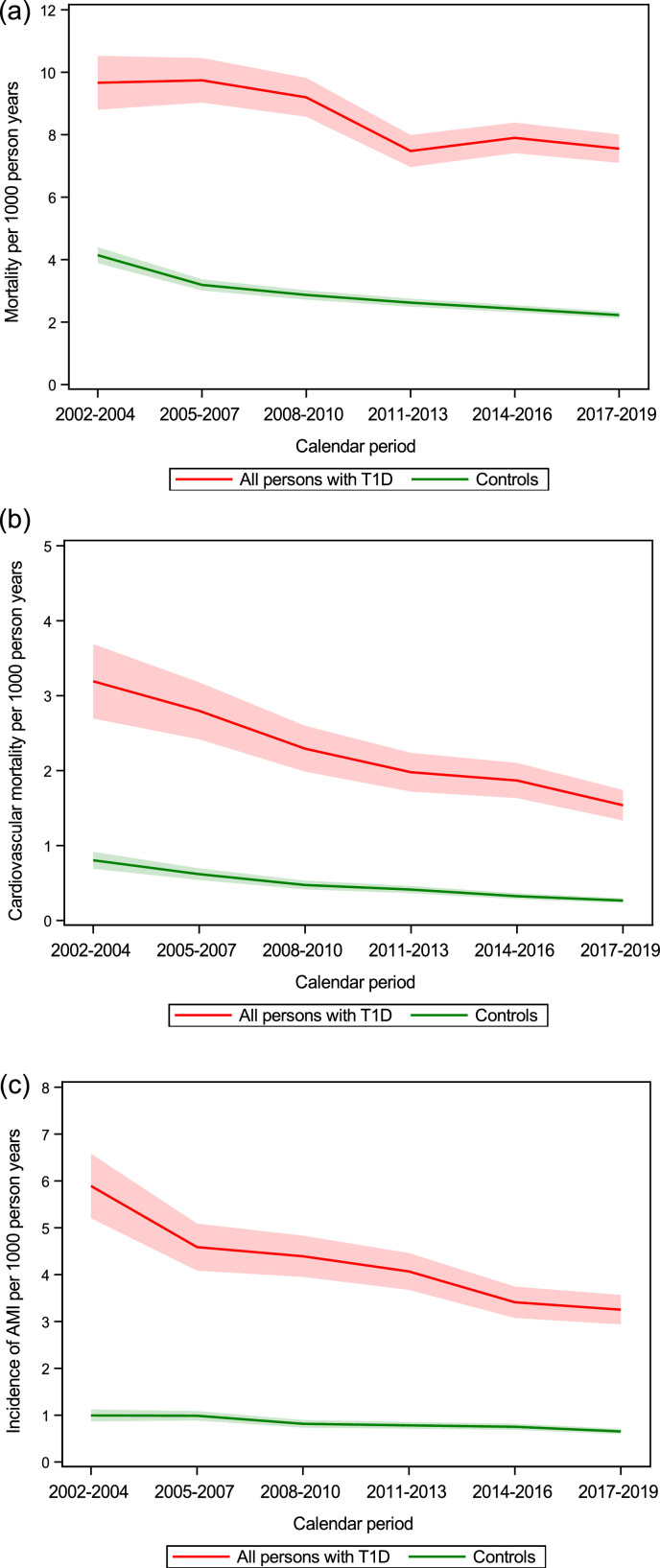
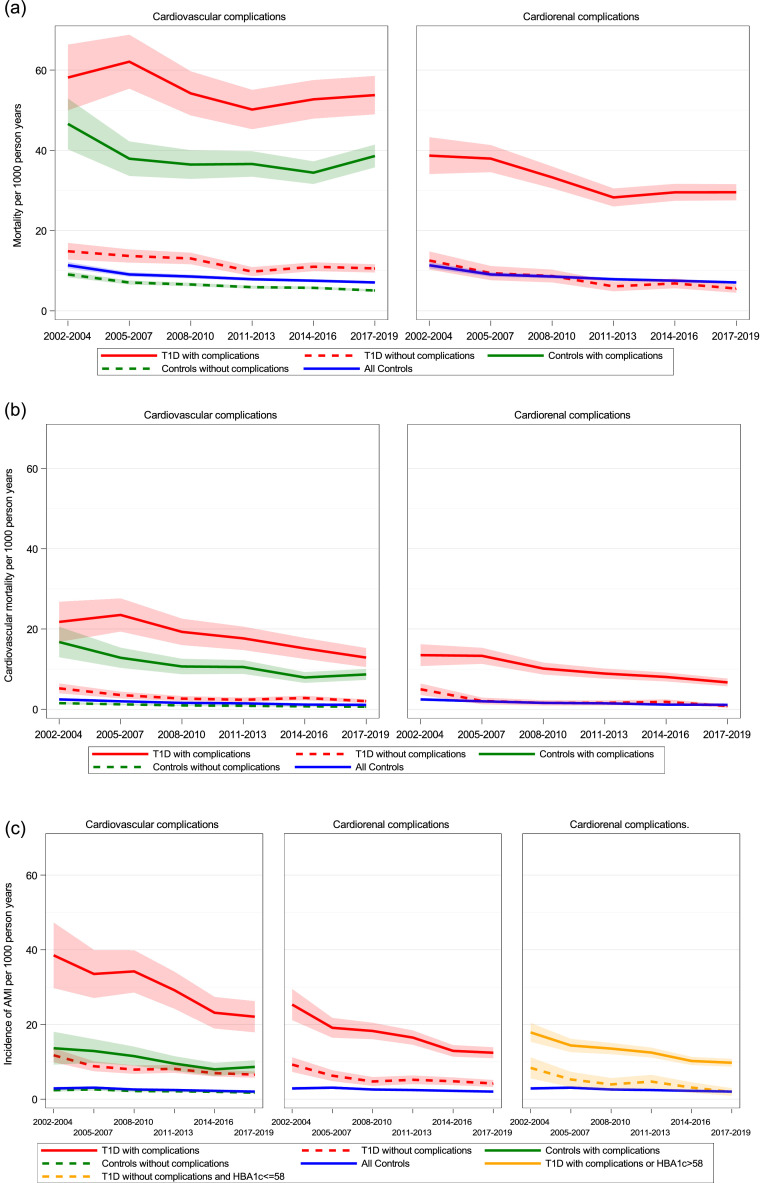
Findings: Mean age in persons with T1D was 32.4 years and 44.9% (20,446/45,575) were women. Age- and sex- adjusted mortality rates declined over time in both groups but remained significantly higher in those with T1D compared to controls during 2017-2019, 7.62 (95% CI 7.16; 8·08) vs. 2.23 (95% CI 2.13; 2.33) deaths per 1,000 person years. Myocardial infarction, heart failure and stroke decreased over time in both groups, with persistent excess risks in the range of 3.4-5.0 times from 2017 to 2019 in those with T1D. T1D persons ≥45 years without previous renal or cardiovascular complications had standardized mortality rates similar or even lower than controls 5.55 (4.51; 6.60) vs.7.08 (6.75; 7.40) respectively in the last time period.
Interpretation: Excess mortality persisted over time in persons with T1D, largely in patients with cardiorenal complications. Improved secondary prevention with a focus on individualized treatment is needed to close the gap in mortality for individuals with T1D.
Funding: This study was financed by grants from the ALF-agreement, NovoNordisk Foundation and the Swedish Heart and Lung Foundation.
Keywords: Acute myocardial infarction; Heart failure; Ischemic heart disease; Stroke; Type 1 diabetes.
© 2022 The Authors.
Conflict of interest statement
HW has served on safety or advisory boards for ScanCLAD, SweVAD and Xvivo. MOW has served on advisory boards or lectured for MSD, Lilly, Novo Nordisk, and Sanofi, and has organized a professional regional meeting sponsored by Eli Lilly, Rubin Medical, Sanofi, Novartis, and Novo Nordisk. MAP has Research Grant Support from Novartis and has been a consultant to AstraZeneca, Boehringer Ingelheim, Eli Lilly Alliance, Corvidia, DalCor, GlaxoSmithKline, Lexicon, NHLBI CONNECTs (Master Protocol Committee), Novartis, Novo Nordisk, Peerbridge and Sanofi; and has equity in DalCor. ML has received research grants from Eli Lilly and Novonordisk and been a consultant or received honoraria from Astra Zeneca, Boehringer Ingelheim, Eli Lilly and Novonordisk. No other potential conflicts of interest relevant to this article were reported.
Figures
References
LinkOut - more resources
Full Text Sources
Miscellaneous
