

Bronchiolitis obliterans syndrome after lung or haematopoietic stem cell transplantation: current management and future directions
- PMID: 35898810
- PMCID: PMC9309343
- DOI: 10.1183/23120541.00185-2022
Bronchiolitis obliterans syndrome after lung or haematopoietic stem cell transplantation: current management and future directions
Abstract
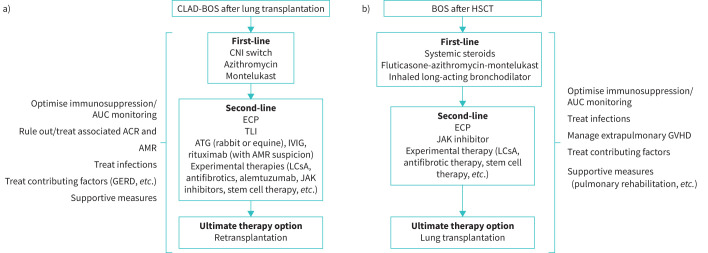
Bronchiolitis obliterans syndrome (BOS) may develop after either lung or haematopoietic stem cell transplantation (HSCT), with similarities in histopathological features and clinical manifestations. However, there are differences in the contributory factors and clinical trajectories between the two conditions. BOS after HSCT occurs due to systemic graft-versus-host disease (GVHD), whereas BOS after lung transplantation is limited to the lung allograft. BOS diagnosis after HSCT is more challenging, as the lung function decline may occur due to extrapulmonary GVHD, causing sclerosis or inflammation in the fascia or muscles of the respiratory girdle. Treatment is generally empirical with no established effective therapies. This review provides rare insights and commonalities of both conditions, which are not well elaborated elsewhere in contemporary literature, and highlights the importance of cross disciplinary learning from experts in other transplant modalities. Treatment algorithms for each condition are presented, based on the published literature and consensus clinical opinion. Immunosuppression should be optimised, and other conditions or contributory factors treated where possible. When initial treatment fails, the ultimate therapeutic option is lung transplantation (or re-transplantation in the case of BOS after lung transplantation) in carefully selected candidates. Novel therapies under investigation include aerosolised liposomal cyclosporine, Janus kinase inhibitors, antifibrotic therapies and (in patients with BOS after lung transplantation) B-cell-directed therapies. Effective novel treatments that have a tangible impact on survival and thereby avoid the need for lung transplantation or re-transplantation are urgently required.
Copyright ©The authors 2022.
Conflict of interest statement
Conflict of interest: A.R. Glanville has received an honorarium for an advisory role from Zambon and is chair of the Zambon DSMB for the Boston trials. Conflict of interest: G.M. Verleden has received an honorarium for an advisory role from Zambon. Conflict of interest: M. Perch has received an honorarium for an advisory role from Zambon, a research grant (institutional) from Roche, speaker fees from Novartis, GSK and Therakos, and other financial support from Boehringer. Conflict of interest: E.D. Lease has received an honorarium for an advisory role from Zambon. Conflict of interest: G-S. Cheng has received an honorarium for an advisory role from Zambon. Conflict of interest: A. Bergeron has received an honorarium for an advisory role from Zambon. Conflict of interest: C. Benden has received an honorarium for an advisory role from Zambon and speaker fees from Therakos. Conflict of interest: J. Gottlieb has received an honorarium for advisory roles from Zambon, research grants from Zambon and Deutsche Forschungsgemeinschaft, and advisory funding from Theravance, Merck and Altara. Conflict of interest: J.L. Todd has received an honorarium for an advisory role from Zambon, Altavant and Natera, and research grants (institutional) from Boehringer Ingelheim, AstraZeneca and CareDx. Conflict of interest: K.M. Williams has received an honorarium for an advisory role from Zambon.
Figures
References
-
- Krishna R, Anjum F, Oliver TI. Bronchiolitis Obliterans. Treasure Island, FL, StatPearls, 2020. - PubMed
Publication types
LinkOut - more resources
Full Text Sources