

Chemoprophylactic Anticoagulation 72 Hours After Spinal Fracture Surgical Treatment Decreases Venous Thromboembolic Events Without Increasing Surgical Complications
- PMID: 35898944
- PMCID: PMC9309228
- DOI: 10.1016/j.xnsj.2022.100141
Chemoprophylactic Anticoagulation 72 Hours After Spinal Fracture Surgical Treatment Decreases Venous Thromboembolic Events Without Increasing Surgical Complications
Abstract
Background: Prophylactic anticoagulation is commonly used following operative treatment of spinal fractures to prevent Venous Thromboembolism (VTE) but carries a risk of bleeding complications. The purpose of the study was to compare VTE and bleeding complications for MID (≤72h) versus LATE (>72h) chemoprophylaxis timing after spinal fracture operative intervention.
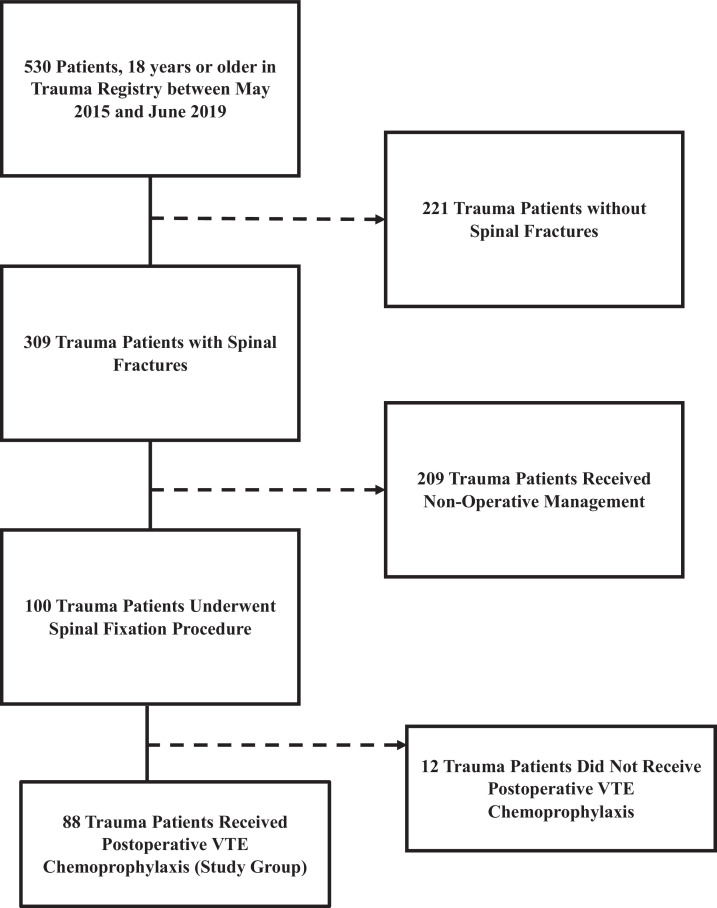
Methods: This is a retrospective review of patients treated for spinal fractures that received anticoagulation chemoprophylaxis between May 2015 and June 2019. Chemoprophylaxis initiation timing (MID vs. LATE) was the primary grouping variable. Patients with traumatic brain injury or evidence of intracranial or intraspinal bleed were excluded. Demographics, injury mechanisms, operative procedures, timing of administration of VTE prophylaxis, Injury Severity Score (ISS) and Spine Abbreviated Injury Scale (AIS), and complications including VTE and bleeding complications were collected. Predictors of VTE were identified using a binary logistic regression.
Results: Eighty-eight patients (65M, 23F) met inclusion criteria. The median age was 55 years, and median Injury Severity Score (ISS) was 14. MID had 68 patients and LATE had 20. Nine patients developed VTE (6 LATE, 3 MID, p<0.01). Three patients developed bleeding complications, and all occurred in the LATE group (p=0.01). ISS (p<0.01) and GCS (p<0.01) also correlated with an increased VTE rate.
Conclusions: Chemoprophylactic anticoagulation at 72 hours in surgically treated spinal fracture patients demonstrates a lower VTE rate without increasing complications. VTE prophylaxis can be initiated at 72 hours following spine fixation to decrease postinjury morbidity and mortality in this high-risk patient population.
Keywords: Bleeding Complications; Deep Venous Thrombosis; Epidural Hematoma; Intervention; Prophylactic Anticoagulation; Spinal Fracture; Venous Thromboembolism.
© 2022 The Author(s).
Conflict of interest statement
None.
Figures
Similar articles
-
Impact of venous thromboembolism chemoprophylaxis on postoperative hemorrhage following operative stabilization of spine fractures.J Trauma Acute Care Surg. 2017 Dec;83(6):1108-1113. doi: 10.1097/TA.0000000000001640. J Trauma Acute Care Surg. 2017. PMID: 28697027
-
Early pharmacological venous thromboembolism prophylaxis is safe after operative fixation of traumatic spine fractures.Spine (Phila Pa 1976). 2015 Mar 1;40(5):299-304. doi: 10.1097/BRS.0000000000000754. Spine (Phila Pa 1976). 2015. PMID: 25901977
-
Timing and risks of chemoprophylaxis after spinal surgery: a single-center experience with 6869 consecutive patients.J Neurosurg Spine. 2017 Dec;27(6):681-693. doi: 10.3171/2017.3.SPINE161076. Epub 2017 Sep 8. J Neurosurg Spine. 2017. PMID: 28885127
-
Chemical prophylaxis and venous thromboembolism following elective spinal surgery: A systematic review and meta-analysis.N Am Spine Soc J. 2023 Nov 23;17:100295. doi: 10.1016/j.xnsj.2023.100295. eCollection 2024 Mar. N Am Spine Soc J. 2023. PMID: 38204918 Free PMC article. Review.
-
Chemoprophylaxis for venous thromboembolism in pelvic and/or acetabular fractures: A systematic review.Injury. 2022 Apr;53(4):1449-1454. doi: 10.1016/j.injury.2022.01.045. Epub 2022 Feb 5. Injury. 2022. PMID: 35148902
Cited by
-
Postoperative Timing of Chemoprophylaxis and Its Impact on Thromboembolism and Bleeding Following Major Abdominal Surgery: A Multicenter Cohort Study.World J Surg. 2023 May;47(5):1174-1183. doi: 10.1007/s00268-023-06899-5. Epub 2023 Feb 18. World J Surg. 2023. PMID: 36806555 Free PMC article.
-
Saudi Critical Care Society clinical practice guidelines on the prevention of venous thromboembolism in adults with trauma: reviewed for evidence-based integrity and endorsed by the Scandinavian Society of Anaesthesiology and Intensive Care Medicine.Ann Intensive Care. 2023 May 11;13(1):41. doi: 10.1186/s13613-023-01135-8. Ann Intensive Care. 2023. PMID: 37165105 Free PMC article. Review.
-
Anatomic distribution and analysis of influencing factors on deep vein thrombosis in patients with spinal fractures caused by high-energy injuries.Eur J Trauma Emerg Surg. 2025 Mar 7;51(1):128. doi: 10.1007/s00068-025-02801-1. Eur J Trauma Emerg Surg. 2025. PMID: 40053113
-
Timing of Chemical Anticoagulant Administration in Spine Trauma and its Impact on VTE, Bleeding, and Mortality: A Systematic Review and Meta-Analysis.Global Spine J. 2025 Jul 6:21925682251353138. doi: 10.1177/21925682251353138. Online ahead of print. Global Spine J. 2025. PMID: 40619341 Free PMC article. Review.
-
Commentary on "Chemoprophylactic anticoagulation 72 hours after spinal fracture surgical treatment decreases venous thromboembolic events without increasing surgical complications".N Am Spine Soc J. 2022 Oct 25;12:100179. doi: 10.1016/j.xnsj.2022.100179. eCollection 2022 Dec. N Am Spine Soc J. 2022. PMID: 36589693 Free PMC article. No abstract available.
References
-
- New P.W., et al. Estimating the incidence and prevalence of traumatic spinal cord injury in Australia. Archives of physical medicine and rehabilitation. 2015;96(1):76–83. - PubMed
-
- Pearson A.M., et al. C2 vertebral fractures in the Medicare population: incidence, outcomes, and costs. JBJS. 2016;98(6):449–456. - PubMed
-
- Tator C., et al. Comparison of surgical and conservative management in 208 patients with acute spinal cord injury. Canadian journal of neurological sciences. 1987;14:60–69. S1. - PubMed
-
- Donovan W. Operative and nonoperative management of spinal cord injury. A review. Spinal Cord. 1994;32(6):375–388. - PubMed
LinkOut - more resources
Full Text Sources
Miscellaneous
