

Introducing antimicrobial stewardship to the outpatient clinics of a suburban academic health system
- PMID: 35899218
- PMCID: PMC9319114
- DOI: 10.1017/ash.2021.228
Introducing antimicrobial stewardship to the outpatient clinics of a suburban academic health system
Abstract
Objective: To establish an antimicrobial stewardship program in the outpatient setting.
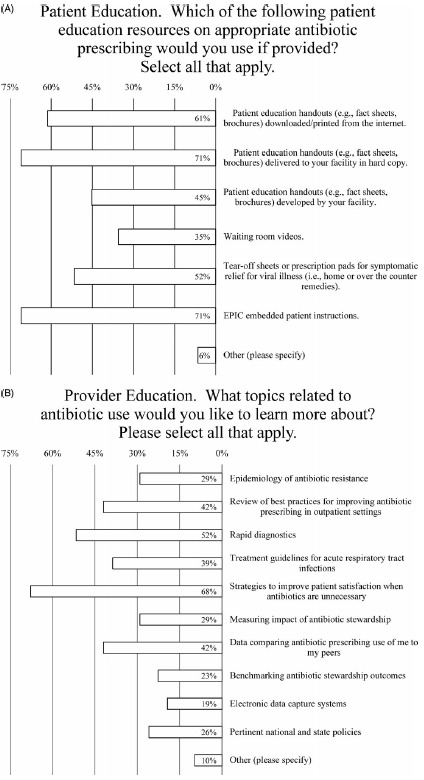
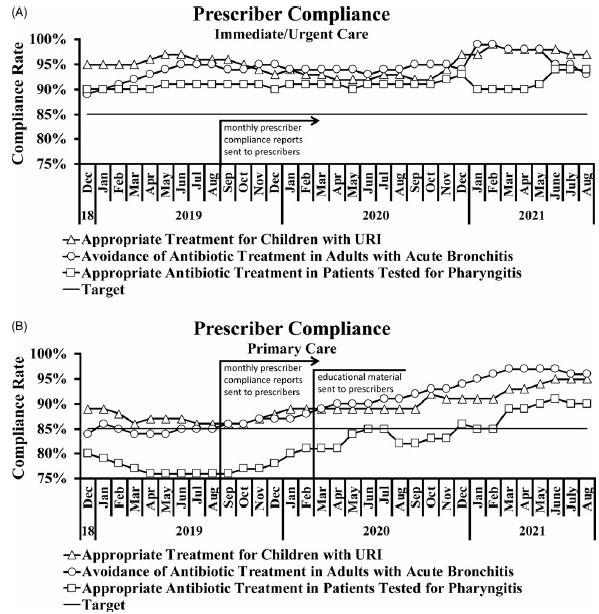
Design: Prescribers of antimicrobials were asked to complete a survey regarding antimicrobial stewardship. We also monitored their compliance with appropriate prescribing practices, which were shared in monthly quality improvement reports.
Setting: The study was performed at Loyola University Health System, an academic teaching healthcare system in a metropolitan suburban environment.
Participants: Prescribers of antimicrobials across 19 primary care and 3 immediate- and urgent-care clinics.
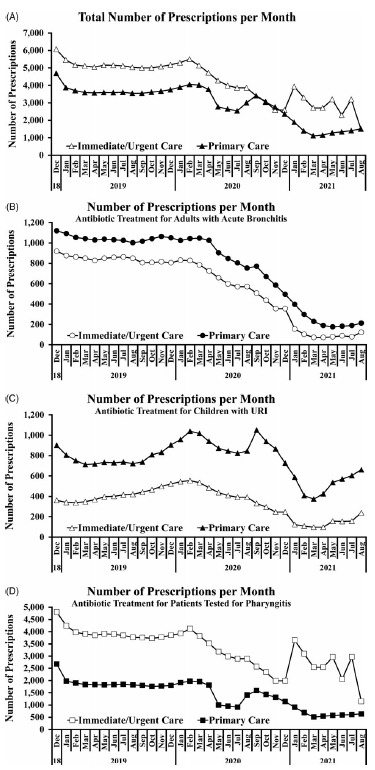
Methods: The voluntary survey was developed using SurveyMonkeyand was distributed via e-mail. Data were collected anonymously. Rates of compliance with appropriate prescribing practices were abstracted from electronic health records and assessed by 3 metrics: (1) avoidance of antibiotics in adult acute bronchitis and appropriate antibiotic treatment in (2) patients tested for pharyngitis and (3) children with upper respiratory tract infections.
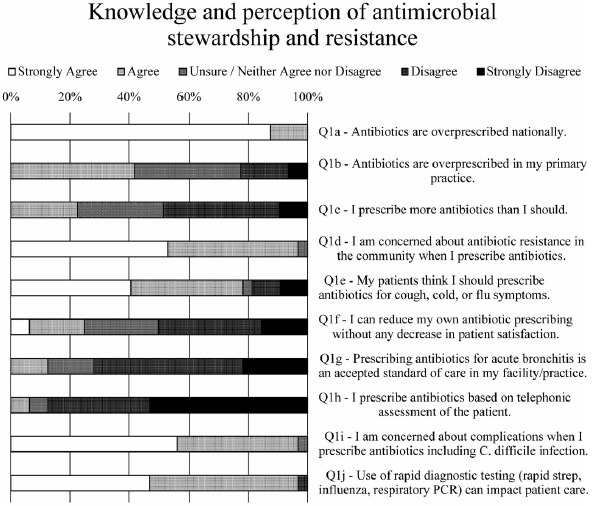
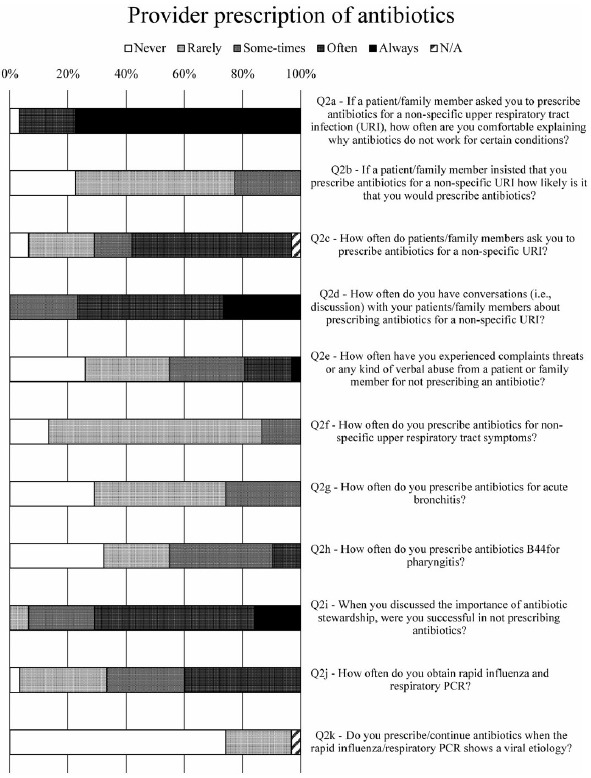
Results: Prescribers were highly knowledgeable about what constitutes appropriate prescribing; verified compliance rates were highly concordant with self-reported rates. Nearly all prescribers were concerned about resistance, but fewer than half believed antibiotics were overprescribed in their office. Among respondents, 74% reported intense pressure from patients to prescribe antimicrobials inappropriately. Immediate- and urgent-care prescribers had higher rates of compliance than primary-care prescribers, and the latter group responded well to monthly reports and online educational resources.
Conclusions: Intense pressure from patients to prescribe antimicrobials when they are not indicated leads to overprescribing, an effect compounded by the importance of patient satisfaction scores. Compliance reporting improved the number of appropriate antibiotics prescribed in the primary care setting.
Conflict of interest statement
Conflicts of interest. All authors report no conflicts of interest relevant to this article.
Figures
Similar articles
-
Pharmacist-Driven Transitions of Care Practice Model for Prescribing Oral Antimicrobials at Hospital Discharge.JAMA Netw Open. 2022 May 2;5(5):e2211331. doi: 10.1001/jamanetworkopen.2022.11331. JAMA Netw Open. 2022. PMID: 35536577 Free PMC article.
-
Antibiotic Prescriptions for Upper Respiratory Infections in a Pediatric Office Versus an Urgent Care Center.Glob Pediatr Health. 2019 Mar 15;6:2333794X19835632. doi: 10.1177/2333794X19835632. eCollection 2019. Glob Pediatr Health. 2019. PMID: 30906818 Free PMC article.
-
Do family medicine residents optimally prescribe antibiotics for common infectious conditions seen in a primary care setting?J Assoc Med Microbiol Infect Dis Can. 2023 Nov 29;8(3):192-200. doi: 10.3138/jammi-2022-0042. eCollection 2023 Nov. J Assoc Med Microbiol Infect Dis Can. 2023. PMID: 38058504 Free PMC article.
-
Behavioral Economics and Ambulatory Antibiotic Stewardship: A Narrative Review.Clin Ther. 2021 Oct;43(10):1654-1667. doi: 10.1016/j.clinthera.2021.08.004. Epub 2021 Oct 23. Clin Ther. 2021. PMID: 34702589 Free PMC article. Review.
-
Navigating performance measures for ambulatory antimicrobial stewardship: a review of HEDIS® and other metrics the steward should know.Antimicrob Steward Healthc Epidemiol. 2024 Dec 13;4(1):e217. doi: 10.1017/ash.2024.468. eCollection 2024. Antimicrob Steward Healthc Epidemiol. 2024. PMID: 39758875 Free PMC article. Review.
Cited by
-
Leveraging Health Systems to Expand and Enhance Antibiotic Stewardship in Outpatient Settings.Jt Comm J Qual Patient Saf. 2024 Apr;50(4):289-295. doi: 10.1016/j.jcjq.2023.10.007. Epub 2023 Oct 21. Jt Comm J Qual Patient Saf. 2024. PMID: 37968193 Free PMC article. No abstract available.
References
-
- Penicillin’s finder assays its future. New York Times June 26, 1945.
-
- Centers for Disease Control and Prevention. Outpatient antibiotic prescriptions—United States. Atlanta: CDC; 2014.
-
- Dyar O, Huttner B, Schouten J, Pulcini C. What is antimicrobial stewardship? Clin Microbiol Infect 2017; 23: 793–798. - PubMed
-
- McGregor JC, Fitzpatrick MA, Suda KJ. Expanding antimicrobial stewardship through quality improvement. JAMA Netw Open 2021;4:e211072. - PubMed
Grants and funding
LinkOut - more resources
Full Text Sources