

Clinical Importance of the Persistent Primitive Trigeminal Artery in Vascular Lesions and Its Role in Endovascular Treatment
- PMID: 35899260
- PMCID: PMC9309485
- DOI: 10.3389/fneur.2022.928608
Clinical Importance of the Persistent Primitive Trigeminal Artery in Vascular Lesions and Its Role in Endovascular Treatment
Abstract
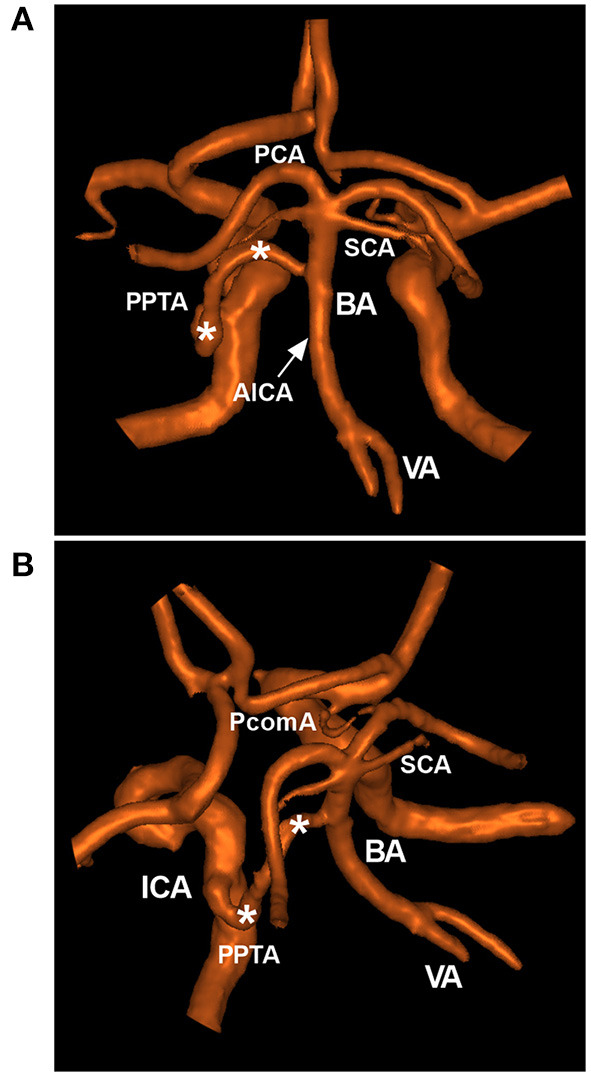
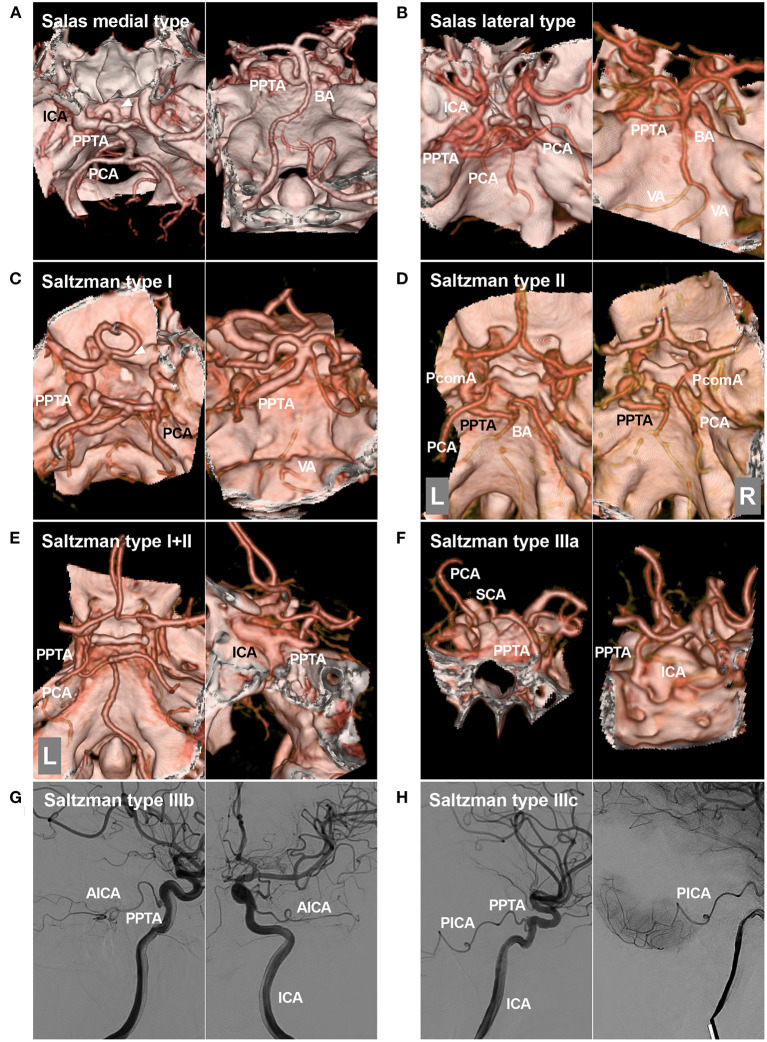
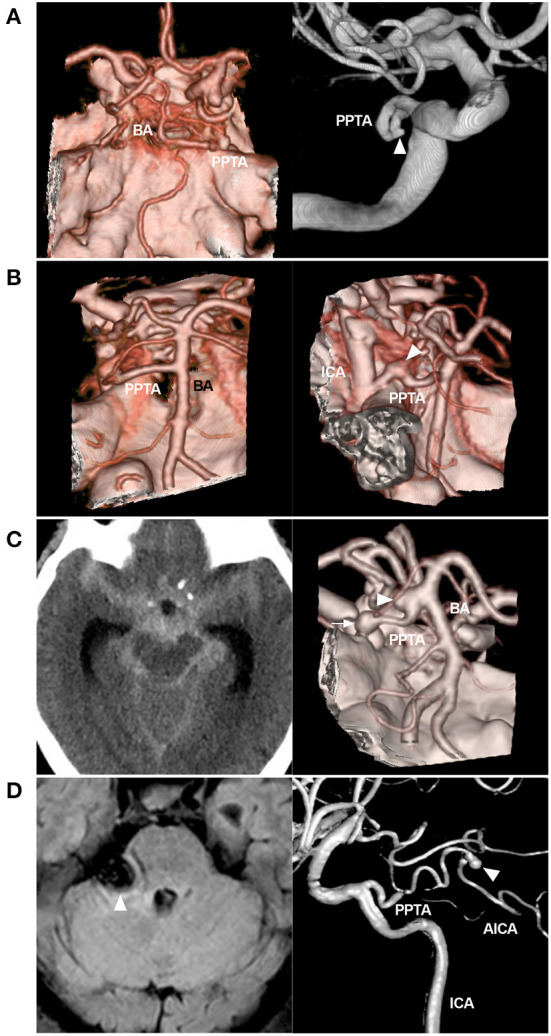
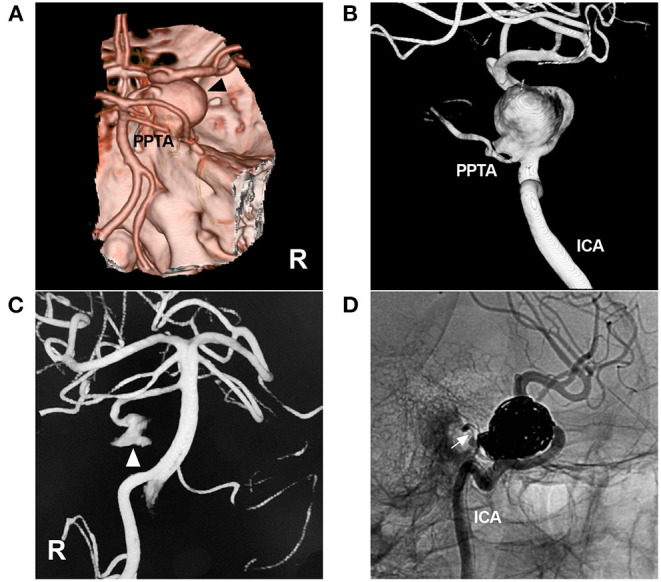
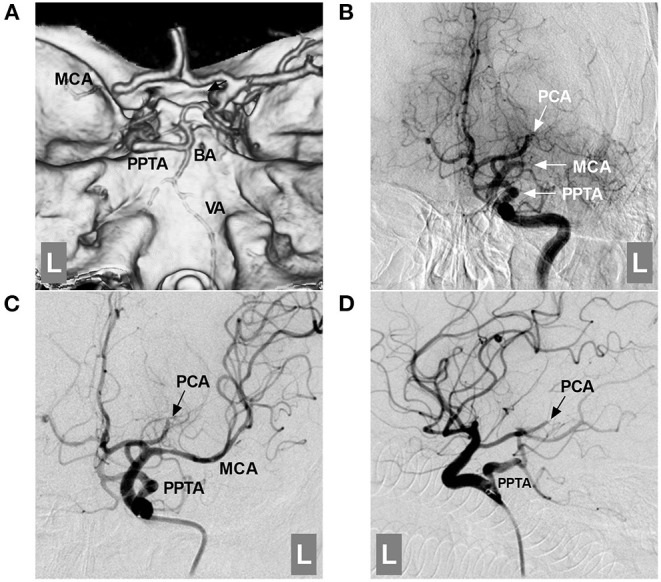
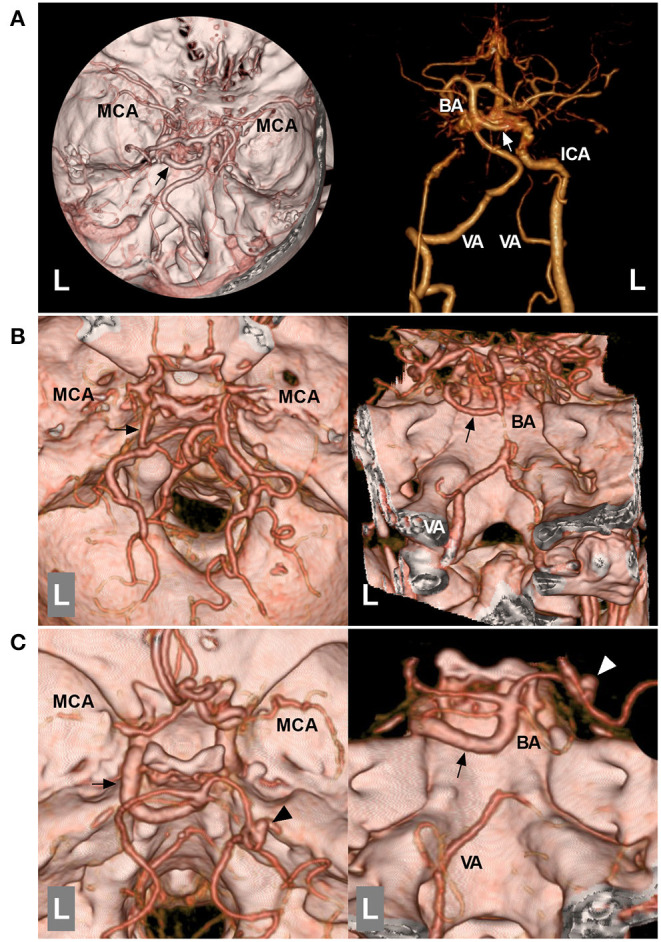
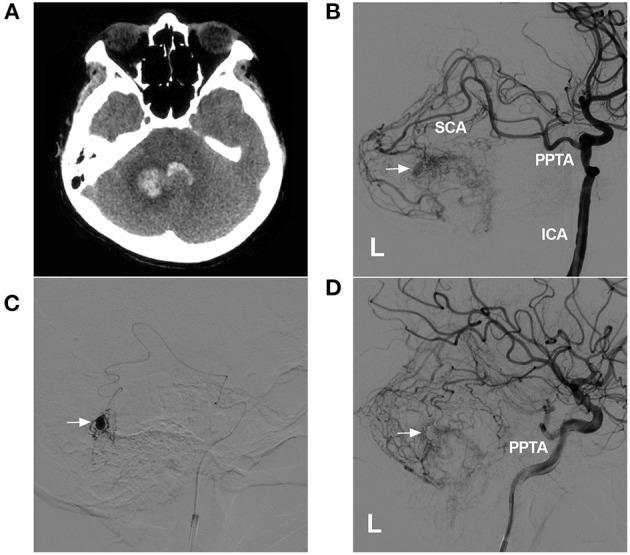
The persistent primitive trigeminal artery (PPTA) extends from the internal carotid artery to the basilar artery between the origins of the anterior inferior cerebellar artery and superior cerebellar artery. PPTAs have complex anatomical characteristics. Salas and Saltzman classifications are most often used in PPTAs. The PPTA can play many roles in vascular lesions, including intracranial aneurysms, brain arteriovenous malformations, trigeminal artery-cavernous fistulas, Moyamoya disease, and large vessel occlusion. For these lesions, surgical treatment is difficult due to the deep location and complex anatomy of the PPTA, but endovascular treatment (EVT) has emerged as a good alternative. Currently, a complete review of the clinical importance of the PPTA in terms of its role in the development and EVT of vascular lesions is lacking. Therefore, we conducted a PubMed search, performed a review of the relevant extracted literature and cataloged our experience with PPTAs. By review, we found that a thorough understanding of the anatomical and angiographic features of this PPTA is of utmost importance when making therapeutic decisions for any of these pathological conditions.
Keywords: clinical importance; endovascular treatment; persistent primitive trigeminal artery; review; vascular lesion.
Copyright © 2022 Wang and Yu.
Conflict of interest statement
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Figures
Similar articles
-
Carotid-cavernous Fistula Associated with a Ruptured Persistent Primitive Trigeminal Artery Aneurysm: A Case Report and Review of Literature.NMC Case Rep J. 2021 Oct 16;8(1):691-696. doi: 10.2176/nmccrj.cr.2021-0084. eCollection 2021. NMC Case Rep J. 2021. PMID: 35079535 Free PMC article.
-
Coexistence of Persistent Primitive Trigeminal Artery, Moyamoya Disease, and Multiple Intracranial Aneurysms: A Case Report and Literature Review.World Neurosurg. 2019 Apr;124:313-318. doi: 10.1016/j.wneu.2019.01.030. Epub 2019 Jan 24. World Neurosurg. 2019. PMID: 30684717
-
Persistent primitive trigeminal artery: a review.Turk Neurosurg. 2012;22(4):399-406. doi: 10.5137/1019-5149.JTN.4427-11.1. Turk Neurosurg. 2012. PMID: 22843453 Review.
-
Treatment of Aneurysms in Persistent Primitive Trigeminal Arteries with Stent-Assisted Coil Embolization.J Neuroendovasc Ther. 2021;15(3):150-156. doi: 10.5797/jnet.cr.2020-0049. Epub 2020 Sep 21. J Neuroendovasc Ther. 2021. PMID: 37502730 Free PMC article.
-
Spontaneous Persistent Primitive Trigeminal Artery-Cavernous Sinus Fistula Successfully Treated by Multipronged Coil Embolization: Case Report and Literature Review.World Neurosurg. 2019 Aug;128:122-126. doi: 10.1016/j.wneu.2019.05.003. Epub 2019 May 10. World Neurosurg. 2019. PMID: 31078800 Review.
Cited by
-
Anatomical insights and clinical implications of the persistent trigeminal artery: A cadaveric study utilizing latex injection techniques.Surg Neurol Int. 2025 Mar 28;16:103. doi: 10.25259/SNI_1084_2024. eCollection 2025. Surg Neurol Int. 2025. PMID: 40206769 Free PMC article.
-
The Relationship between the Permanent Trigeminal Artery and Cerebrovascular Disease: A Meta-Analysis.Iran J Public Health. 2024 May;53(5):988-996. doi: 10.18502/ijph.v53i5.15579. Iran J Public Health. 2024. PMID: 38912150 Free PMC article. Review.
-
Case Report: Endovascular electrothrombosis treatment for carotid cavernous fistula caused by ruptured primitive trigeminal artery aneurysm.Front Surg. 2025 Mar 21;12:1559977. doi: 10.3389/fsurg.2025.1559977. eCollection 2025. Front Surg. 2025. PMID: 40191284 Free PMC article.
-
Subarachnoid hemorrhage secondary to Chiari 1 malformation in a patient presenting with recurrent severe headache: A case report, imaging, and anatomic considerations.Surg Neurol Int. 2025 Jul 18;16:292. doi: 10.25259/SNI_374_2025. eCollection 2025. Surg Neurol Int. 2025. PMID: 40837325 Free PMC article.
-
Fenestrations of cerebral arteries and their correlation with brain aneurysms.Front Neuroanat. 2025 Mar 26;19:1523305. doi: 10.3389/fnana.2025.1523305. eCollection 2025. Front Neuroanat. 2025. PMID: 40206441 Free PMC article.
References
-
- Padget DH. The development of the cranial arteries in the human embryo. Contrib Embryol. (1948) 32:205–62.
Publication types
LinkOut - more resources
Full Text Sources