

The personality traits activity, self-reproach, and negative affect jointly predict clinical recurrence, depressive symptoms, and low quality of life in inflammatory bowel disease patients
- PMID: 35900592
- PMCID: PMC9596530
- DOI: 10.1007/s00535-022-01902-7
The personality traits activity, self-reproach, and negative affect jointly predict clinical recurrence, depressive symptoms, and low quality of life in inflammatory bowel disease patients
Abstract
Background: The bidirectional "gut-brain axis" has been implicated in the pathogenesis of inflammatory bowel diseases (IBD). While the influence of stress and depressive symptoms on IBD is well-characterized, the role of personality remains insufficiently investigated.
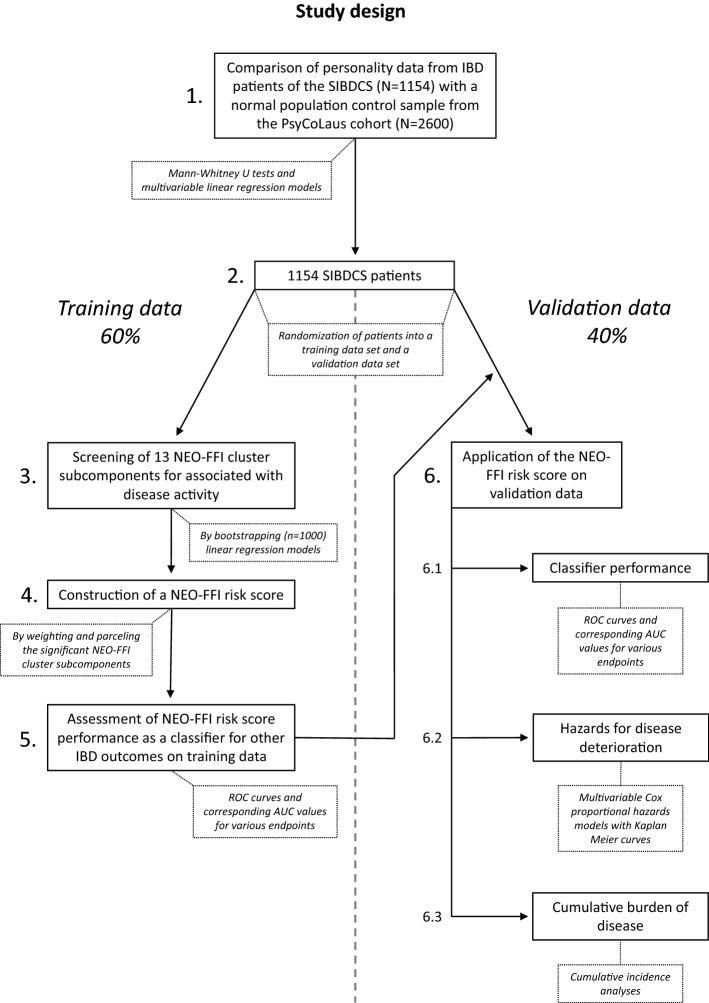
Methods: Personality was assessed in 1154 Swiss IBD cohort study (SIBDCS) patients via the NEO-Five-Factor Inventory (NEO-FFI) as well as in 2600 participants of the population-based CoLaus¦PsyCoLaus cohort study (NEO-FFI-revised). The NEO-FFI subcomponents activity, self-reproach and negative affect were associated with higher IBD disease activity and were combined to a NEO-FFI risk score. This risk score was validated and its effect on clinical IBD course and psychological endpoints was analysed in time-to-event and cumulative incidence analyses.
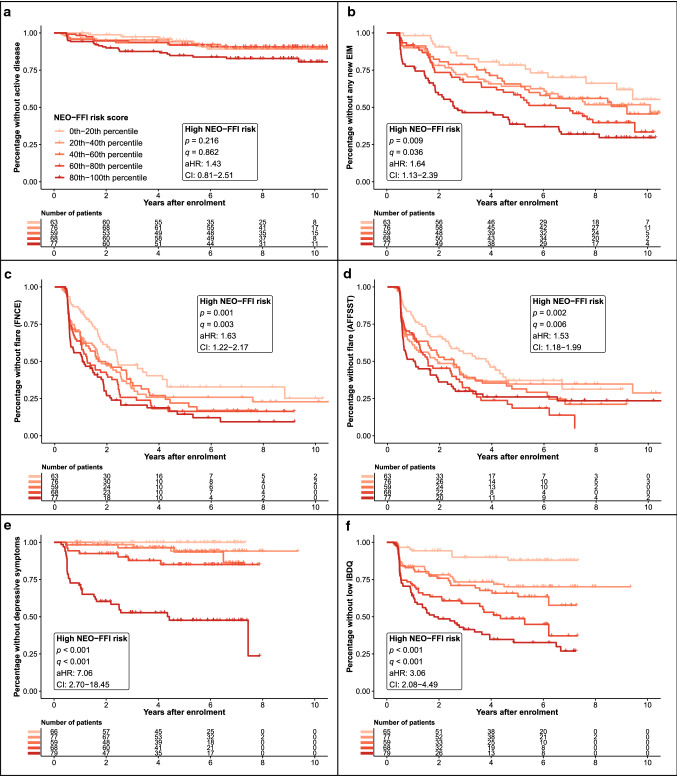
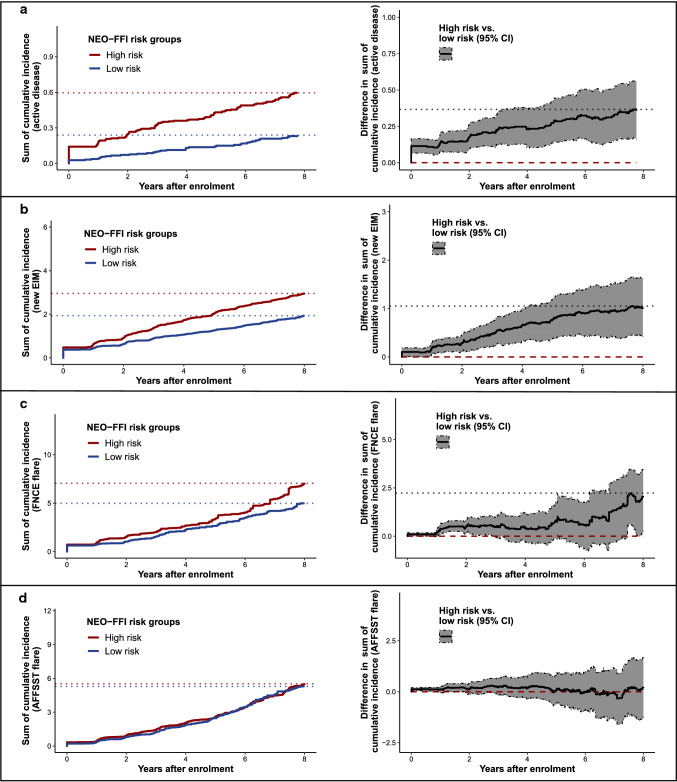
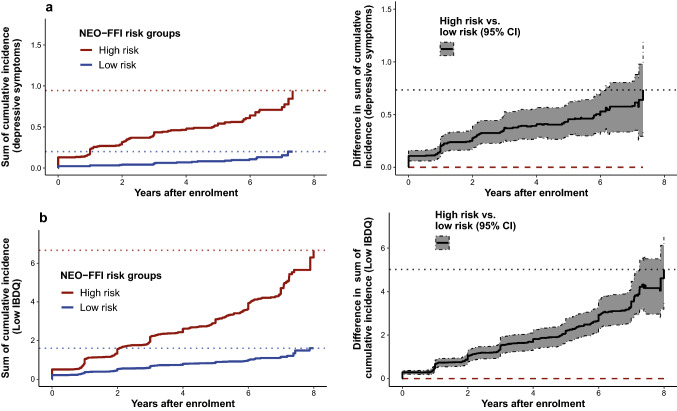
Results: In time-to-event analyses, a high NEO-FFI risk score was predictive for the clinical endpoints of new extraintestinal manifestation [EIM, adjusted hazard ratio (aHR) = 1.64, corrected p value (q) = 0.036] and two established composite flare endpoints (aHR = 1.53-1.63, q = 0.003-0.006) as well as for the psychological endpoints depressive symptoms (aHR = 7.06, q < 0.001) and low quality of life (aHR = 3.06, q < 0.001). Furthermore, cumulative incidence analyses showed that patients at high NEO-FFI risk experienced significantly more episodes of active disease, new EIMs, one of the flare endpoints, depressive episodes and low disease-related quality of life. Personalities of IBD patients showed only minor differences from the general population sample (Pearson's r = 0.03-0.14).
Conclusions: Personality assessed by the NEO-FFI contained considerable predictive power for disease recurrence, depressive symptoms and low quality of life in IBD patients. Nevertheless, the personalities of IBD patients did not substantially differ from the general population.
Keywords: Five-factor model; Flares; IBD; NEO-FFI; Personality.
© 2022. The Author(s).
Conflict of interest statement
S.B.U.J., B.M.L., J.W., B.A., B.Y., N.K. M.P. and S.B. have nothing to disclose. T.G. reports consultant fees from Pfizer and Takeda, honorary fees from Abbvie, Falk Pharma and Janssen, and travel grants from Falk Pharma and Vifor.P.S. reports consultant fees from Pfizer, Takeda, Janssen-Cilag and Abbvie.L.B. reports fees for consulting/advisory board from Abbvie, MSD, Vifor, Falk, Esocap, Calypso, Ferring, Pfizer, Shire, Takeda, Janssen, Ewopharma. TG has consulting contracts with Sanofi-Regeneron and Falk Pharma GmbH, received travel grants from Falk Pharma GmbH and Vifor, and an unrestricted research grant from Novartis.R.v.K. has served on an advisory board of Vifor AG, Switzerland unrelated to this work. G.R. has consulted Abbvie, Augurix, BMS, Boehringer, Calypso, Celgene, FALK, Ferring, Fisher, Genentech, Gilead, Janssen, MSD, Novartis, Pfizer, Phadia, Roche, UCB, Takeda, Tillots, Vifor, Vital Solutions and Zeller. G.R. has received speaker's honoraria from Astra Zeneca, Abbvie, FALK, Janssen, MSD, Pfizer, Phadia, Takeda, Tillots, UCB, Vifor and Zeller. G.R. has received educational grants and research grants from Abbvie, Ardeypharm, Augurix, Calypso, FALK, Flamentera, MSD, Novartis, Pfizer, Roche, Takeda, Tillots, UCB and Zeller. B.M. has served at an advisory board for Gilead, Takeda, BMS, iQONE and Novigenix. He has received speaking fees from Vifor, MSD and Takeda and traveling fees from Vifor, Novartis, MSD and Takeda. BM has received research grants from MSD and BMS unrelated to this work.
Figures

References
Publication types
MeSH terms
Grants and funding
- 33CS30-148422/Schweizerischer Nationalfonds zur Förderung der Wissenschaftlichen Forschung
- 3200B0-105993/Schweizerischer Nationalfonds zur Förderung der Wissenschaftlichen Forschung
- 3200B0-118308/Schweizerischer Nationalfonds zur Förderung der Wissenschaftlichen Forschung
- 33CSCO-122661/Schweizerischer Nationalfonds zur Förderung der Wissenschaftlichen Forschung
- 33CS30-139468/Schweizerischer Nationalfonds zur Förderung der Wissenschaftlichen Forschung
