

First-emerging islet autoantibody and glucose metabolism: search for type 1 diabetes subtypes
- PMID: 35900772
- PMCID: PMC9422255
- DOI: 10.1530/EC-21-0632
First-emerging islet autoantibody and glucose metabolism: search for type 1 diabetes subtypes
Abstract
Objective: Subtypes in type 1 diabetes pathogenesis have been implicated based on the first-appearing autoantibody (primary autoantibody). We set out to describe the glucose metabolism in preclinical diabetes in relation to the primary autoantibody in children with HLA-conferred disease susceptibility.
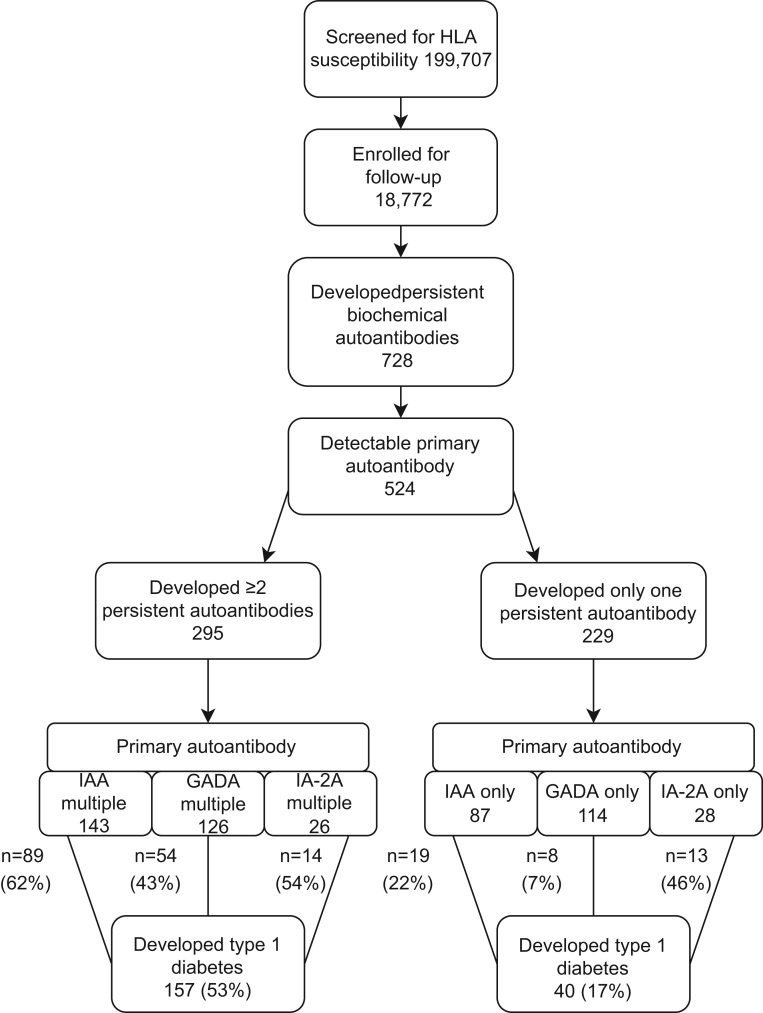
Design and methods: Dysglycemic markers are defined as a 10% increase in HbA1c in a 3-12 months interval or HbA1c ≥5.9% (41 mmol/mol) in two consecutive samples, impaired fasting glucose or impaired glucose tolerance, or a random plasma glucose value ≥7.8 mmol/L. A primary autoantibody could be detected in 295 children who later developed at least 1 additional biochemical autoantibody. These children were divided into three groups: insulin autoantibody (IAA) multiple (n = 143), GAD antibody (GADA) multiple (n = 126) and islet antigen 2 antibody (IA-2A) multiple (n = 26). Another 229 children seroconverted to positivity only for a single biochemical autoantibody and were grouped as IAA only (n = 87), GADA only (n = 114) and IA-2A only (n = 28).
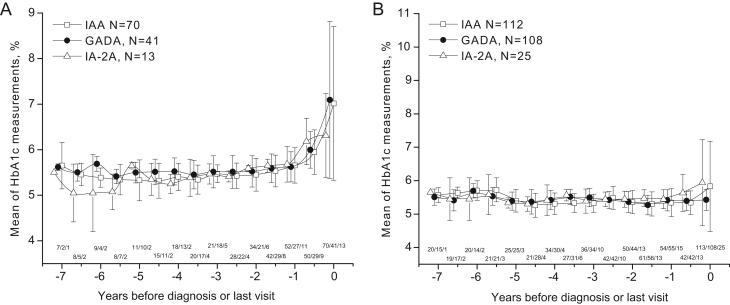
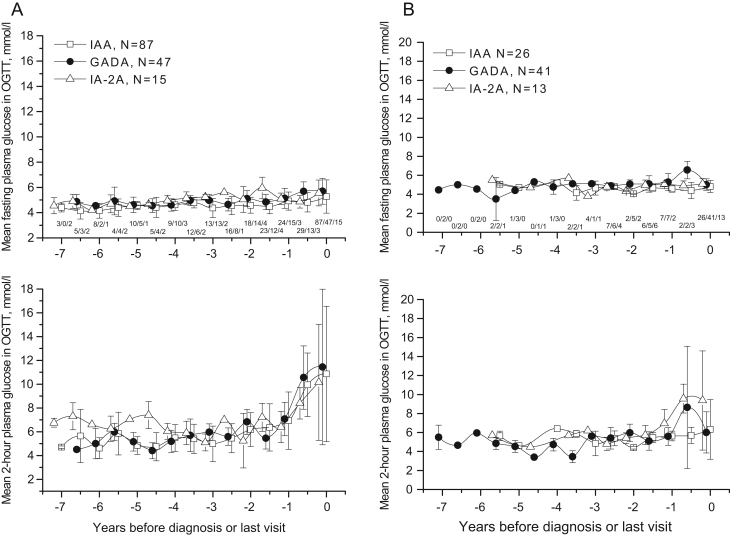
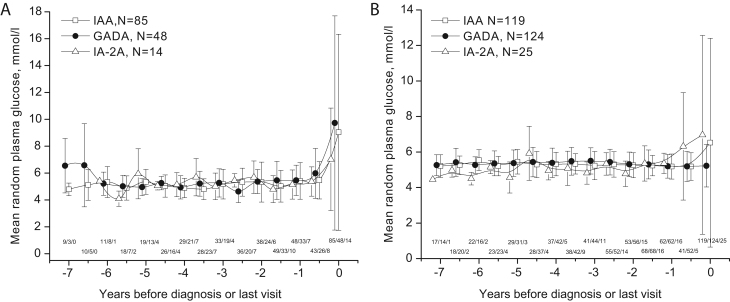
Results: No consistent differences were observed in selected autoantibody groups during the preclinical period. At diagnosis, children with IAA only showed the highest HbA1c (P < 0.001 between groups) and the highest random plasma glucose (P = 0.005 between groups). Children with IA-2A only progressed to type 1 diabetes as frequently as those with IA-2A multiple (46% vs 54%, P = 0.297) whereas those with IAA only or GADA only progressed less often than children with IAA multiple or GADA multiple (22% vs 62% (P < 0.001) and 7% vs 43% (P < 0.001)), respectively.
Conclusions: The phenotype of preclinical diabetes defined by the primary autoantibody is not associated with any discernible differences in glucose metabolism before the clinical disease manifestation.
Keywords: dysglycemia; glucose metabolism; islet autoantibodies; preclinical type 1 diabetes; type 1 diabetes.
Figures
References
-
- Steck AK, Larsson HE, Liu X, Veijola R, Toppari J, Hagopian WA, Haller MJ, Ahmed S, Akolkar B, Lernmark Ået al.Residual beta-cell function in diabetes children followed and diagnosed in the TEDDY study compared to community controls. Pediatric Diabetes 201718794–802. (10.1111/pedi.12485) - DOI - PMC - PubMed
LinkOut - more resources
Full Text Sources
Research Materials
