

An evolutionary machine learning algorithm for cardiovascular disease risk prediction
- PMID: 35901181
- PMCID: PMC9333440
- DOI: 10.1371/journal.pone.0271723
An evolutionary machine learning algorithm for cardiovascular disease risk prediction
Abstract
Introduction: This study developed a novel risk assessment model to predict the occurrence of cardiovascular disease (CVD) events. It uses a Genetic Algorithm (GA) to develop an easy-to-use model with high accuracy, calibrated based on the Isfahan Cohort Study (ICS) database.
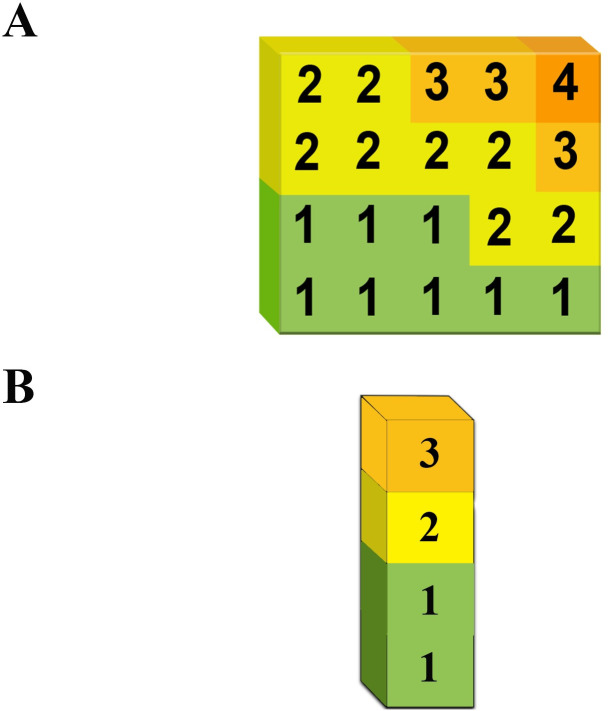
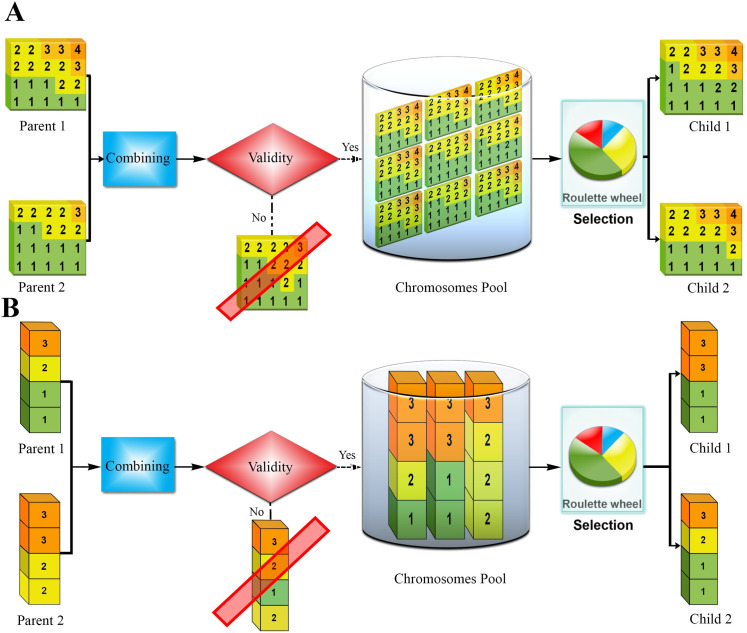
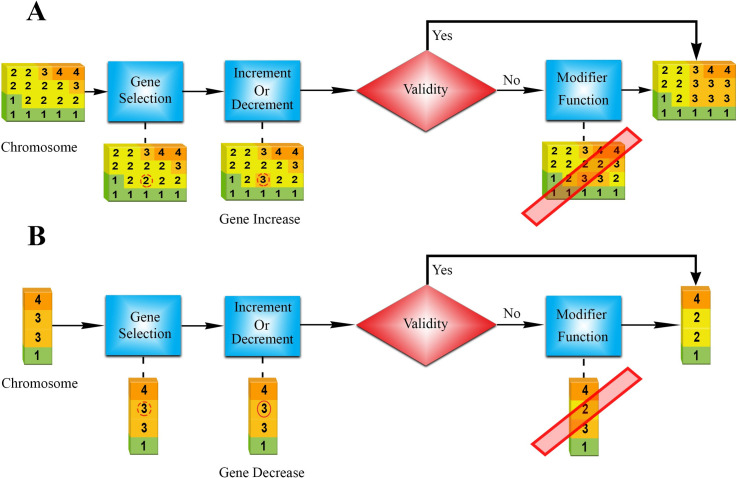
Methods: The ICS was a population-based prospective cohort study of 6,504 healthy Iranian adults aged ≥ 35 years followed for incident CVD over ten years, from 2001 to 2010. To develop a risk score, the problem of predicting CVD was solved using a well-designed GA, and finally, the results were compared with classic machine learning (ML) and statistical methods.
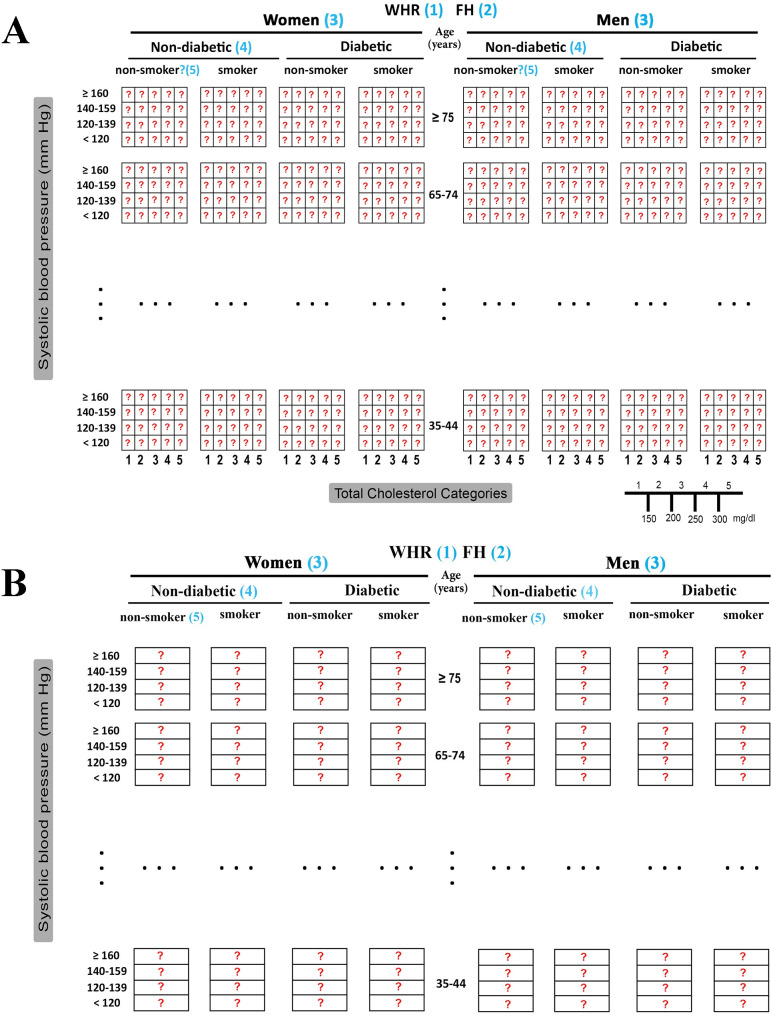
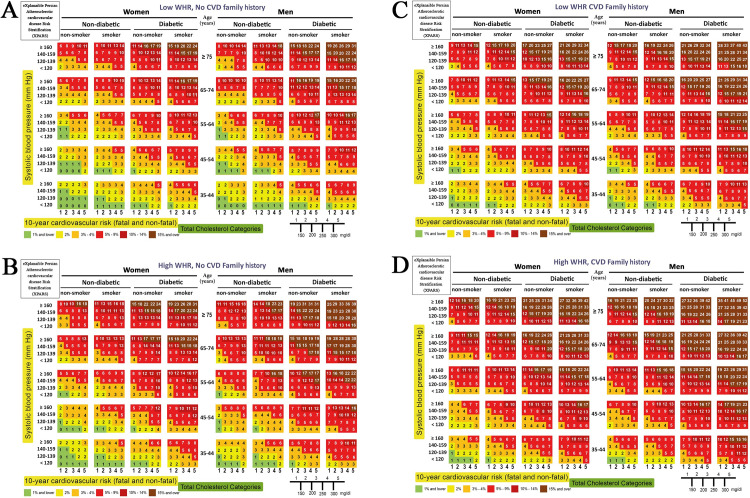
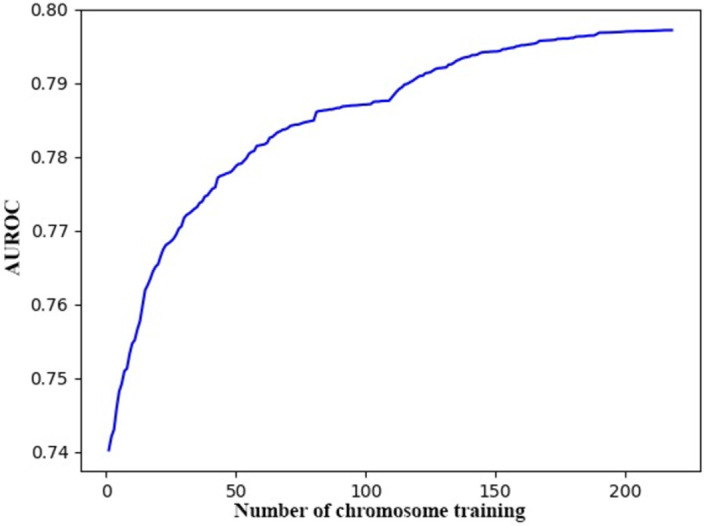
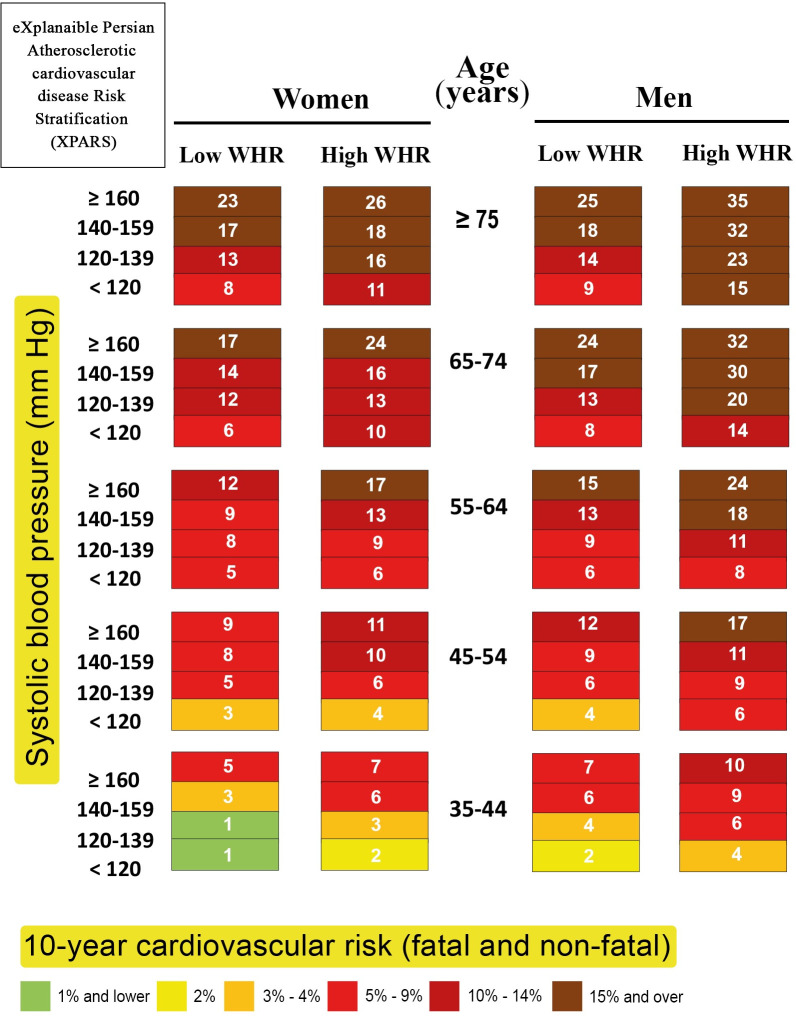
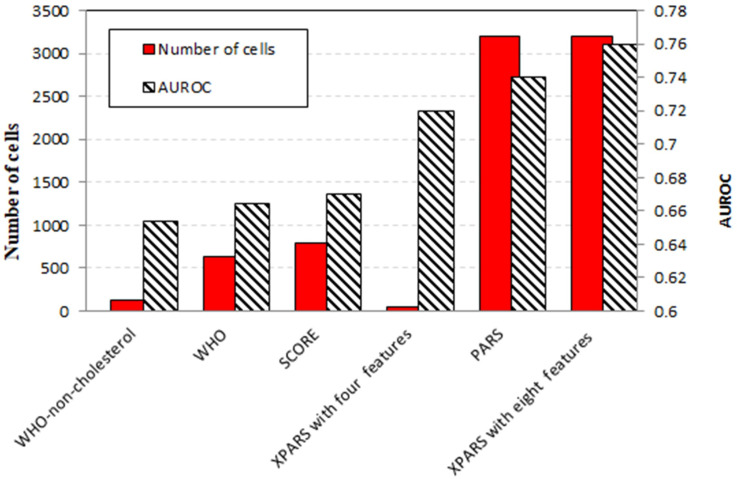
Results: A number of risk scores such as the WHO, and PARS models were utilized as the baseline for comparison due to their similar chart-based models. The Framingham and PROCAM models were also applied to the dataset, with the area under a Receiver Operating Characteristic curve (AUROC) equal to 0.633 and 0.683, respectively. However, the more complex Deep Learning model using a three-layered Convolutional Neural Network (CNN) performed best among the ML models, with an AUROC of 0.74, and the GA-based eXplanaible Persian Atherosclerotic CVD Risk Stratification (XPARS) showed higher performance compared to the statistical methods. XPARS with eight features showed an AUROC of 0.76, and the XPARS with four features, showed an AUROC of 0.72.
Conclusion: A risk model that is extracted using GA substantially improves the prediction of CVD compared to conventional methods. It is clear, interpretable and can be a suitable replacement for conventional statistical methods.
Conflict of interest statement
The authors have declared that no competing interests exist.
Figures
References
-
- Goff DC, Lloyd-Jones DM, Bennett G, Coady S, D’agostino RB, Gibbons R, et al.. 2013 ACC/AHA guideline on the assessment of cardiovascular risk: a report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines. Journal of the American College of Cardiology. 2014;63(25 Part B):2935–59. doi: 10.1161/01.cir.0000437741.48606.98 - DOI - PMC - PubMed
-
- Malcolm S, Dorvil M, Zou B, DeGennaro V. Estimating 10-year cardiovascular disease risk in urban and rural populations in Haiti. Clinical Epidemiology and Global Health. 2020;8(4):1134–9. doi: 10.1016/j.cegh.2020.04.004 - DOI
-
- Bajpai V. The Challenges Confronting Public Hospitals in India, Their Origins, and Possible Solutions. Advances in Public Health. 2014;2014:898502. doi: 10.1155/2014/898502 - DOI
MeSH terms
Associated data
LinkOut - more resources
Full Text Sources
Miscellaneous
