

Determinants of RSV epidemiology following suppression through pandemic contact restrictions
- PMID: 35901639
- PMCID: PMC9301974
- DOI: 10.1016/j.epidem.2022.100614
Determinants of RSV epidemiology following suppression through pandemic contact restrictions
Abstract
Introduction: COVID-19 related non-pharmaceutical interventions (NPIs) led to a suppression of RSV circulation in winter 2020/21 in the UK and an off-season resurgence in Summer 2021. We explore how the parameters of RSV epidemiology shape the size and dynamics of post-suppression resurgence and what we can learn about them from the resurgence patterns observed so far.
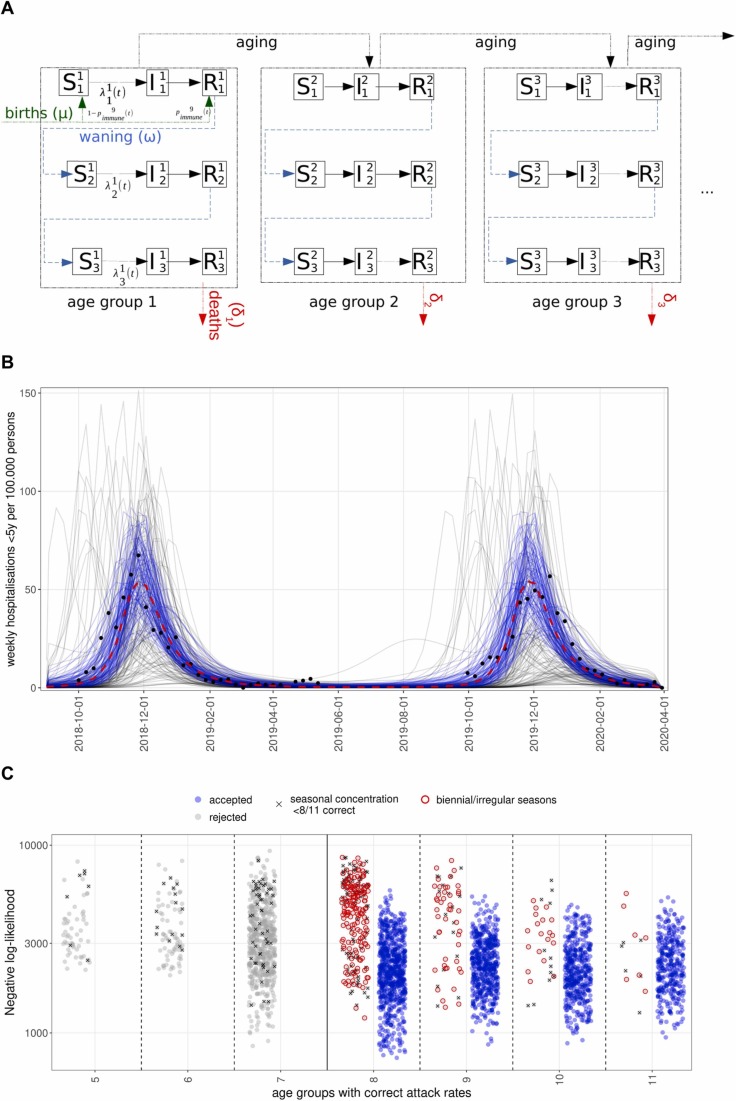
Methods: We developed an age-structured dynamic transmission model of RSV and sampled the parameters governing RSV seasonality, infection susceptibility and post-infection immunity, retaining simulations fitting the UK's pre-pandemic epidemiology by a set of global criteria consistent with likelihood calculations. From Spring 2020 to Summer 2021 we assumed a reduced contact frequency, returning to pre-pandemic levels from Spring 2021. We simulated transmission forwards until 2023 and evaluated the impact of the sampled parameters on the projected trajectories of RSV hospitalisations and compared these to the observed resurgence.
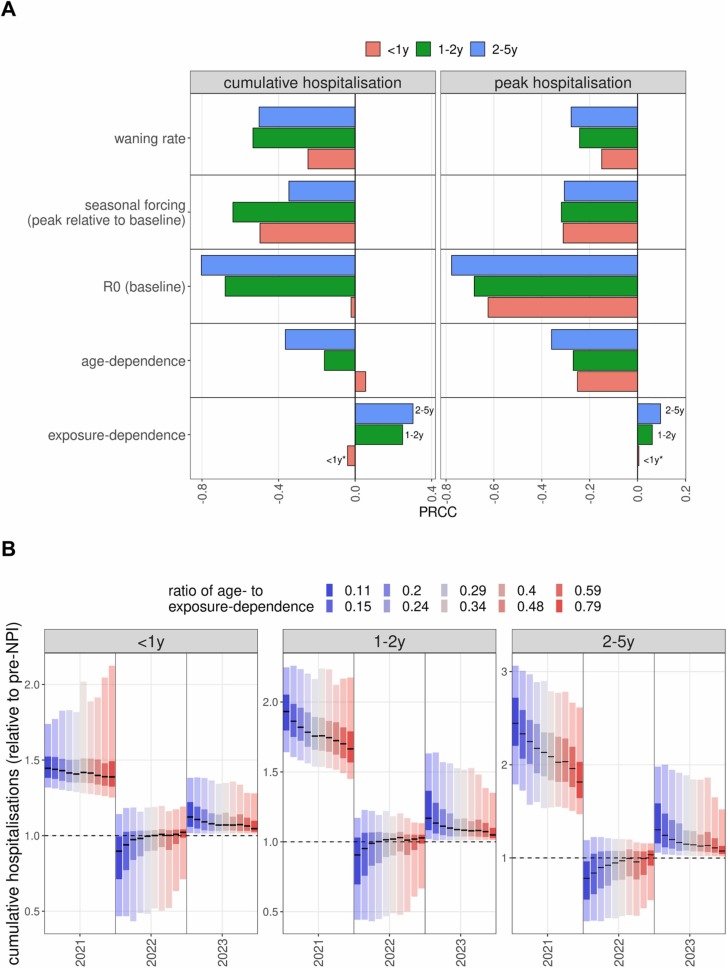
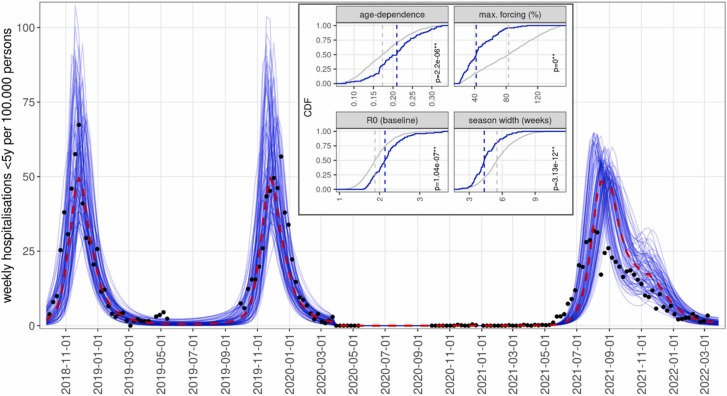
Results: Simulations replicated an out-of-season resurgence of RSV in 2021. If unmitigated, paediatric RSV hospitalisation incidence in the 2021/22 season was projected to increase by 30-60% compared to pre-pandemic levels. The increase was larger if infection risk was primarily determined by immunity acquired from previous exposure rather than age-dependent factors, exceeding 90 % and 130 % in 1-2 and 2-5 year old children, respectively. Analysing the simulations replicating the observed early outbreak in 2021 in addition to pre-pandemic RSV data, we found they were characterised by weaker seasonal forcing, stronger age-dependence of infection susceptibility and higher baseline transmissibility.
Conclusion: COVID-19 mitigation measures in the UK stopped RSV circulation in the 2020/21 season and generated immunity debt leading to an early off-season RSV epidemic in 2021. A stronger dependence of infection susceptibility on immunity from previous exposure increases the size of the resurgent season. The early onset of the RSV resurgence in 2021, its marginally increased size relative to previous seasons and its decline by January 2022 suggest a stronger dependence of infection susceptibility on age-related factors, as well as a weaker effect of seasonality and a higher baseline transmissibility. The pattern of resurgence has been complicated by contact levels still not back to pre-pandemic levels. Further fitting of RSV resurgence in multiple countries incorporating data on contact patterns will be needed to further narrow down these parameters and to better predict the pathogen's future trajectory, planning for a potential expansion of new immunisation products against RSV in the coming years.
Keywords: Disease Dynamics; Epidemiology; Non-pharmaceutical interventions; RSV; Transmission modelling.
Copyright © 2022. Published by Elsevier B.V.
Conflict of interest statement
Conflicts of interest All authors declare that they have no conflicts of interest.
Figures
Similar articles
-
Estimation of the Timing and Intensity of Reemergence of Respiratory Syncytial Virus Following the COVID-19 Pandemic in the US.JAMA Netw Open. 2021 Dec 1;4(12):e2141779. doi: 10.1001/jamanetworkopen.2021.41779. JAMA Netw Open. 2021. PMID: 34913973 Free PMC article.
-
Characterising the changes in RSV epidemiology in Beijing, China during 2015-2023: results from a prospective, multi-centre, hospital-based surveillance and serology study.Lancet Reg Health West Pac. 2024 Mar 27;45:101050. doi: 10.1016/j.lanwpc.2024.101050. eCollection 2024 Apr. Lancet Reg Health West Pac. 2024. PMID: 38699290 Free PMC article.
-
Impact of COVID‑19 pandemic restrictions and subsequent relaxation on the prevalence of respiratory virus hospitalizations in children.BMC Pediatr. 2024 Feb 2;24(1):91. doi: 10.1186/s12887-024-04566-9. BMC Pediatr. 2024. PMID: 38302912 Free PMC article. Review.
-
Epidemiology and viral loads of respiratory syncytial virus in hospitalized children prior to and during COVID-19 pandemic in Hangzhou, China.J Med Virol. 2024 Aug;96(8):e29855. doi: 10.1002/jmv.29855. J Med Virol. 2024. PMID: 39119991
-
Respiratory syncytial virus in children: epidemiology and clinical impact post-COVID-19.Curr Opin Infect Dis. 2023 Dec 1;36(6):522-528. doi: 10.1097/QCO.0000000000000967. Epub 2023 Oct 13. Curr Opin Infect Dis. 2023. PMID: 37830952 Review.
Cited by
-
Trends and Dynamics of Respiratory Viruses in Hospitalized Children of Fuzhou: Insights Into the Impact of COVID-19 Pandemic Control Measures.Int J Gen Med. 2025 Feb 12;18:759-770. doi: 10.2147/IJGM.S511995. eCollection 2025. Int J Gen Med. 2025. PMID: 39963516 Free PMC article.
-
Changes in the global hospitalisation burden of respiratory syncytial virus in young children during the COVID-19 pandemic: a systematic analysis.Lancet Infect Dis. 2024 Apr;24(4):361-374. doi: 10.1016/S1473-3099(23)00630-8. Epub 2023 Dec 20. Lancet Infect Dis. 2024. PMID: 38141633 Free PMC article.
-
[Epidemiological characteristics of respiratory syncytial virus infection in children in Nanchang and its correlation with climate environmental factors].Zhongguo Dang Dai Er Ke Za Zhi. 2024 Dec 15;26(12):1282-1287. doi: 10.7499/j.issn.1008-8830.2406109. Zhongguo Dang Dai Er Ke Za Zhi. 2024. PMID: 39725390 Free PMC article. Chinese.
-
Incidence of Respiratory Syncytial Virus-Associated Lower Respiratory Tract Illness in Infants in Low- and Middle-Income Regions During the Coronavirus Disease 2019 Pandemic.Open Forum Infect Dis. 2023 Dec 1;10(12):ofad553. doi: 10.1093/ofid/ofad553. eCollection 2023 Dec. Open Forum Infect Dis. 2023. PMID: 38088983 Free PMC article.
-
Respiratory Syncytial Virus Hospital-Based Burden of Disease in Children Younger Than 5 Years, 2015-2022.JAMA Netw Open. 2024 Apr 1;7(4):e247125. doi: 10.1001/jamanetworkopen.2024.7125. JAMA Netw Open. 2024. PMID: 38635270 Free PMC article.
References
-
- Chu H.Y., Tielsch J., Katz J., Magaret A.S., Khatry S., LeClerq S.C. Transplacental transfer of maternal respiratory syncytial virus (RSV) antibody and protection against RSV disease in infants in rural Nepal. J. Clin. Virol. Publ. Pan Am. Soc. Clin. Virol. 2017;95:90–95. doi: 10.1016/j.jcv.2017.08.017. - DOI - PMC - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
