

Perioperative outcomes associated with general and spinal anesthesia after total joint arthroplasty for osteoarthritis: a large, Canadian, retrospective cohort study
- PMID: 35902103
- PMCID: PMC9343014
- DOI: 10.1503/cjs.008821
Perioperative outcomes associated with general and spinal anesthesia after total joint arthroplasty for osteoarthritis: a large, Canadian, retrospective cohort study
Abstract
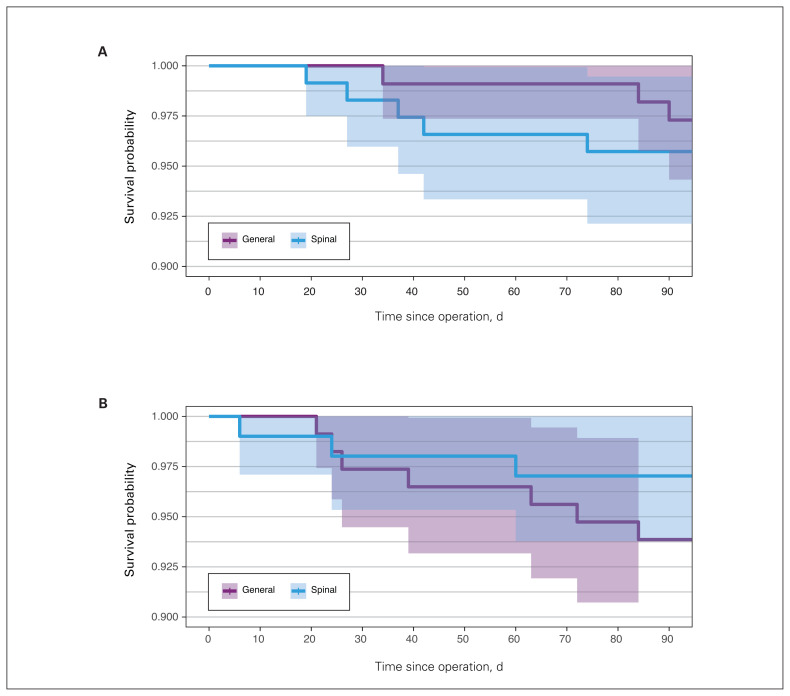
Background: Compared with general anesthesia, spinal anesthesia has many benefits for patients undergoing total hip (THA) or total knee (TKA) arthroplasty, but few studies have explored rates of morbidity and mortality. We aimed to compare perioperative outcomes by anesthetic type for patients undergoing THA or TKA for osteoarthritis.
Methods: We identified patients who underwent primary THA or TKA from the affiliated institute's database. We calculated inpatient, 30-day, 60-day and 90-day mortality rates, as well as 90-day perioperative complications, readmissions and length of stay (LOS). We compared outcomes between groups using logistic regression and propensity-adjusted multivariate analysis.
Results: We included 6100 (52.2%) patients undergoing THA and 5580 (47.8%) undergoing TKA. We found no differences by anesthetic type in mortality rates up to 90 days after surgery. Patients under spinal anesthesia were less likely to need a blood transfusion (THA odds ratio [OR] 0.75, 95% confidence interval [CI] 0.60 to 0.92; TKA OR 0.52, 95% CI 0.40 to 0.67) and were more likely to be discharged home among those who underwent TKA (OR 1.61, 95% CI 1.30 to 2.00). Patients who received spinal anesthesia for THA had a longer LOS (0.28 d, 95% CI 0.17 to 0.39), and patients who received spinal anesthesia for TKA had a shorter LOS than those who received general anesthesia (-0.34 d, 95% CI -0.51 to -0.18). Anesthetic type was not associated with any difference in adverse events.
Conclusion: These findings may inform decisions on anesthetic type for total joint arthroplasty, especially for rapid discharge protocols. Further research is needed to understand postoperative pain and functional outcomes between anesthetic types.
Contexte:: Comparée à l’anesthésie générale, la rachianesthésie présente de nombreux avantages pour les patients subissant une arthroplastie totale de la hanche (ATH) ou du genou (ATG), mais peu d’études se sont intéressées aux taux de morbidité et de mortalité. Nous avons cherché à comparer les résultats périopératoires par type d’anesthésie pour les patients subissant une ATH ou une ATG en raison de l’arthrose.
Méthodes:: Nous avons identifié des patients ayant subi une ATH ou une ATG primaire dans la base de données de l’institut affilié. Nous avons calculé les taux de mortalité des patients hospitalisés, à 30, 60 et 90 jours, ainsi que les complications périopératoires à 90 jours, les réadmissions et la durée de séjour. Nous avons comparé les résultats des différents groupes au moyen d’une analyse de régression logistique et d’une analyse multivariée adaptée au score de propension.
Résultats:: Notre étude comprenait 6100 (52,2 %) patients soumis à une ATH et 5580 (47,8 %) patients soumis à une ATG. Nous n’avons trouvé aucune différence dans les taux de mortalité en fonction du type d’anesthésie jusqu’à 90 jours après l’intervention. Les patients ayant subi la rachianesthésie étaient moins sujets à nécessiter une transfusion sanguine (ATH : rapport des cotes [RC] de 0,75, intervalle de confiance [IC] de 95 % 0,60 à 0,92; ATG : RC de 0,52, IC de 95 % 0,40 à 0,67) et plus sujets à obtenir leur sortie de l’hôpital parmi le groupe des ATG (RC de 1,61, IC de 95 % 1,30 à 2,00). Les patients ayant reçu la rachianesthésie pour l’ATH avaient un séjour de plus longue durée (0,28 j, IC de 95 %, 0,17 à 0,39) et les patients ayant reçu la rachianesthésie pour l’ATG avaient eu un séjour plus court que les patients ayant subi une anesthésie générale (−0,34 j, IC de 95 %, −0,51 à −0,18). Le type d’anesthésie n’était pas associé à une différence dans les événements indésirables.
Conclusion:: Ces résultats peuvent éclairer les décisions sur le type d’anesthésie à privilégier pour les arthroplasties totales, en particulier pour les protocoles de sortie rapide. D’autres recherches sont nécessaires pour comprendre la douleur postopératoire et les résultats fonctionnels propres aux différents types d’anesthésie.
© 2022 CMA Impact Inc. or its licensors.
Conflict of interest statement
Competing interest: Rajrishi Sharma reports consulting fees from Depuy Synthes, Zimmer Biomet, Stryker and OSI. No other competing interests were declared.
Figures
Similar articles
-
Does Hemophilia Increase Risk of Adverse Outcomes Following Total Hip and Knee Arthroplasty? A Propensity Score-Matched Analysis of a Nationwide, Population-Based Study.J Arthroplasty. 2019 Oct;34(10):2329-2336.e1. doi: 10.1016/j.arth.2019.05.062. Epub 2019 Jun 22. J Arthroplasty. 2019. PMID: 31337553
-
Morbidity and Mortality Following Total Hip and Knee Arthroplasty With Spinal Versus General Anesthesia: A Retrospective Analysis.J Arthroplasty. 2024 Nov;39(11):2675-2679. doi: 10.1016/j.arth.2024.04.070. Epub 2024 May 3. J Arthroplasty. 2024. PMID: 38703926
-
Racial Disparities in Outcomes After THA and TKA Are Substantially Mediated by Socioeconomic Disadvantage Both in Black and White Patients.Clin Orthop Relat Res. 2023 Feb 1;481(2):254-264. doi: 10.1097/CORR.0000000000002392. Epub 2022 Sep 14. Clin Orthop Relat Res. 2023. PMID: 36103368 Free PMC article.
-
Factors associated with hospital stay length, discharge destination, and 30-day readmission rate after primary hip or knee arthroplasty: Retrospective Cohort Study.Orthop Traumatol Surg Res. 2019 Sep;105(5):949-955. doi: 10.1016/j.otsr.2019.04.012. Epub 2019 Jun 15. Orthop Traumatol Surg Res. 2019. PMID: 31208932 Review.
-
Racial and Ethnic Disparities in Total Joint Arthroplasty Care: A Contemporary Systematic Review and Meta-Analysis.J Arthroplasty. 2023 Jan;38(1):171-187.e18. doi: 10.1016/j.arth.2022.08.006. Epub 2022 Aug 17. J Arthroplasty. 2023. PMID: 35985539
Cited by
-
Sufentanil sublingual tablet system for enhanced recovery after total knee arthroplasty: a prospective observational case study.Perioper Med (Lond). 2022 Oct 4;11(1):50. doi: 10.1186/s13741-022-00284-x. Perioper Med (Lond). 2022. PMID: 36195919 Free PMC article.
-
Multicenter, prospective cohort study: immediate postoperative gains in active range of motion following robotic-assisted total knee replacement compared to a propensity-matched control using manual instrumentation.Arthroplasty. 2023 Dec 4;5(1):62. doi: 10.1186/s42836-023-00216-0. Arthroplasty. 2023. PMID: 38044446 Free PMC article.
-
Local Infiltration Analgesia Is Superior to Regional Nerve Blocks for Total Hip Arthroplasty: Less Falls, Better Mobility, and Same-Day Discharge.J Clin Med. 2024 Aug 8;13(16):4645. doi: 10.3390/jcm13164645. J Clin Med. 2024. PMID: 39200787 Free PMC article.
References
-
- Lovett-Carter D, Sayeed Z, Abaab L, et al. . Impact of outpatient total joint replacement on postoperative outcomes. Orthop Clin North Am 2018;49:35–44. - PubMed
-
- Sutton JC, III, Antoniou J, Epure LM, et al. . Hospital discharge within 2 days following total hip or knee arthroplasty does not increase major-complication and readmission rates. J Bone Joint Surg Am 2016;98:1419–28. - PubMed
-
- Belmont PJ, Jr, Goodman GP, Waterman BR, et al. . Thirty-day postoperative complications and mortality following total knee arthroplasty: incidence and risk factors among a national sample of 15,321 patients. J Bone Joint Surg Am 2014;96:20–6. - PubMed
-
- Perlas A, Chan VWS, Beattie S. Anesthesia technique and mortality after total hip or knee arthroplasty: a retrospective, propensity score–matched cohort study. Anesthesiology 2016;125:724–31. - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Medical