

Automated multidimensional deep learning platform for referable diabetic retinopathy detection: a multicentre, retrospective study
- PMID: 35902186
- PMCID: PMC9341185
- DOI: 10.1136/bmjopen-2021-060155
Automated multidimensional deep learning platform for referable diabetic retinopathy detection: a multicentre, retrospective study
Abstract
Objective: To develop and validate a real-world screening, guideline-based deep learning (DL) system for referable diabetic retinopathy (DR) detection.
Design: This is a multicentre platform development study based on retrospective, cross-sectional data sets. Images were labelled by two-level certificated graders as the ground truth. According to the UK DR screening guideline, a DL model based on colour retinal images with five-dimensional classifiers, namely image quality, retinopathy, maculopathy gradability, maculopathy and photocoagulation, was developed. Referable decisions were generated by integrating the output of all classifiers and reported at the image, eye and patient level. The performance of the DL was compared with DR experts.
Setting: DR screening programmes from three hospitals and the Lifeline Express Diabetic Retinopathy Screening Program in China.
Participants: 83 465 images of 39 836 eyes from 21 716 patients were annotated, of which 53 211 images were used as the development set and 30 254 images were used as the external validation set, split based on centre and period.
Main outcomes: Accuracy, F1 score, sensitivity, specificity, area under the receiver operating characteristic curve (AUROC), area under the precision-recall curve (AUPRC), Cohen's unweighted κ and Gwet's AC1 were calculated to evaluate the performance of the DL algorithm.
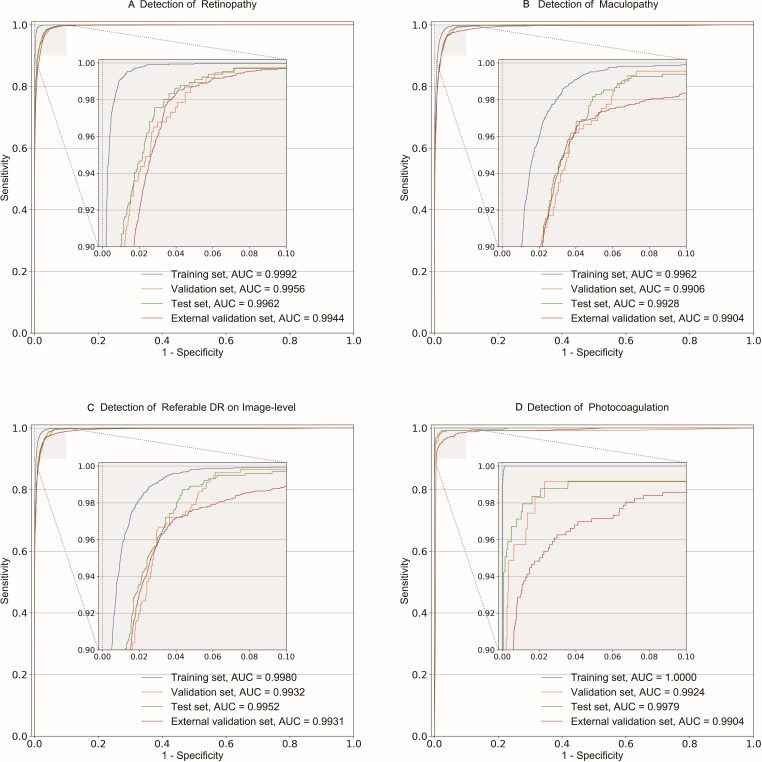
Results: In the external validation set, the five classifiers achieved an accuracy of 0.915-0.980, F1 score of 0.682-0.966, sensitivity of 0.917-0.978, specificity of 0.907-0.981, AUROC of 0.9639-0.9944 and AUPRC of 0.7504-0.9949. Referable DR at three levels was detected with an accuracy of 0.918-0.967, F1 score of 0.822-0.918, sensitivity of 0.970-0.971, specificity of 0.905-0.967, AUROC of 0.9848-0.9931 and AUPRC of 0.9527-0.9760. With reference to the ground truth, the DL system showed comparable performance (Cohen's κ: 0.86-0.93; Gwet's AC1: 0.89-0.94) with three DR experts (Cohen's κ: 0.89-0.96; Gwet's AC1: 0.91-0.97) in detecting referable lesions.
Conclusions: The automatic DL system for detection of referable DR based on the UK guideline could achieve high accuracy in multidimensional classifications. It is suitable for large-scale, real-world DR screening.
Keywords: diabetic retinopathy; medical retina; vetreoretinal.
© Author(s) (or their employer(s)) 2022. Re-use permitted under CC BY-NC. No commercial re-use. See rights and permissions. Published by BMJ.
Conflict of interest statement
Competing interests: None declared.
Figures
Similar articles
-
Development and validation of a 3-D deep learning system for diabetic macular oedema classification on optical coherence tomography images.BMJ Open. 2025 May 31;15(5):e099167. doi: 10.1136/bmjopen-2025-099167. BMJ Open. 2025. PMID: 40449950 Free PMC article.
-
Performance of Automated Machine Learning for Diabetic Retinopathy Image Classification from Multi-field Handheld Retinal Images.Ophthalmol Retina. 2023 Aug;7(8):703-712. doi: 10.1016/j.oret.2023.03.003. Epub 2023 Mar 15. Ophthalmol Retina. 2023. PMID: 36924893
-
Detection of Diabetic Retinopathy from Ultra-Widefield Scanning Laser Ophthalmoscope Images: A Multicenter Deep Learning Analysis.Ophthalmol Retina. 2021 Nov;5(11):1097-1106. doi: 10.1016/j.oret.2021.01.013. Epub 2021 Feb 1. Ophthalmol Retina. 2021. PMID: 33540169
-
Deep learning algorithms for detection of diabetic retinopathy in retinal fundus photographs: A systematic review and meta-analysis.Comput Methods Programs Biomed. 2020 Jul;191:105320. doi: 10.1016/j.cmpb.2020.105320. Epub 2020 Jan 16. Comput Methods Programs Biomed. 2020. PMID: 32088490
-
Performance and Limitation of Machine Learning Algorithms for Diabetic Retinopathy Screening: Meta-analysis.J Med Internet Res. 2021 Jul 3;23(7):e23863. doi: 10.2196/23863. J Med Internet Res. 2021. PMID: 34407500 Free PMC article. Review.
Cited by
-
Risk factors for pupil changes in patients with diabetic retinopathy and cataract after phacoemulsification with intraocular lens implantation.BMC Ophthalmol. 2025 Apr 28;25(1):252. doi: 10.1186/s12886-025-04080-1. BMC Ophthalmol. 2025. PMID: 40295992 Free PMC article.
-
Automated Lung and Colon Cancer Classification Using Histopathological Images.Biomed Eng Comput Biol. 2024 Aug 14;15:11795972241271569. doi: 10.1177/11795972241271569. eCollection 2024. Biomed Eng Comput Biol. 2024. PMID: 39156985 Free PMC article.
-
On the Analyses of Medical Images Using Traditional Machine Learning Techniques and Convolutional Neural Networks.Arch Comput Methods Eng. 2023;30(5):3173-3233. doi: 10.1007/s11831-023-09899-9. Epub 2023 Apr 4. Arch Comput Methods Eng. 2023. PMID: 37260910 Free PMC article.
References
-
- Saeedi P, Petersohn I, Salpea P, et al. . Global and regional diabetes prevalence estimates for 2019 and projections for 2030 and 2045: Results from the International Diabetes Federation Diabetes Atlas, 9th edition. Diabetes Res Clin Pract 2019;157:107843. 10.1016/j.diabres.2019.107843 - DOI - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical