

Prediction algorithm for ICU mortality and length of stay using machine learning
- PMID: 35902633
- PMCID: PMC9334583
- DOI: 10.1038/s41598-022-17091-5
Prediction algorithm for ICU mortality and length of stay using machine learning
Abstract
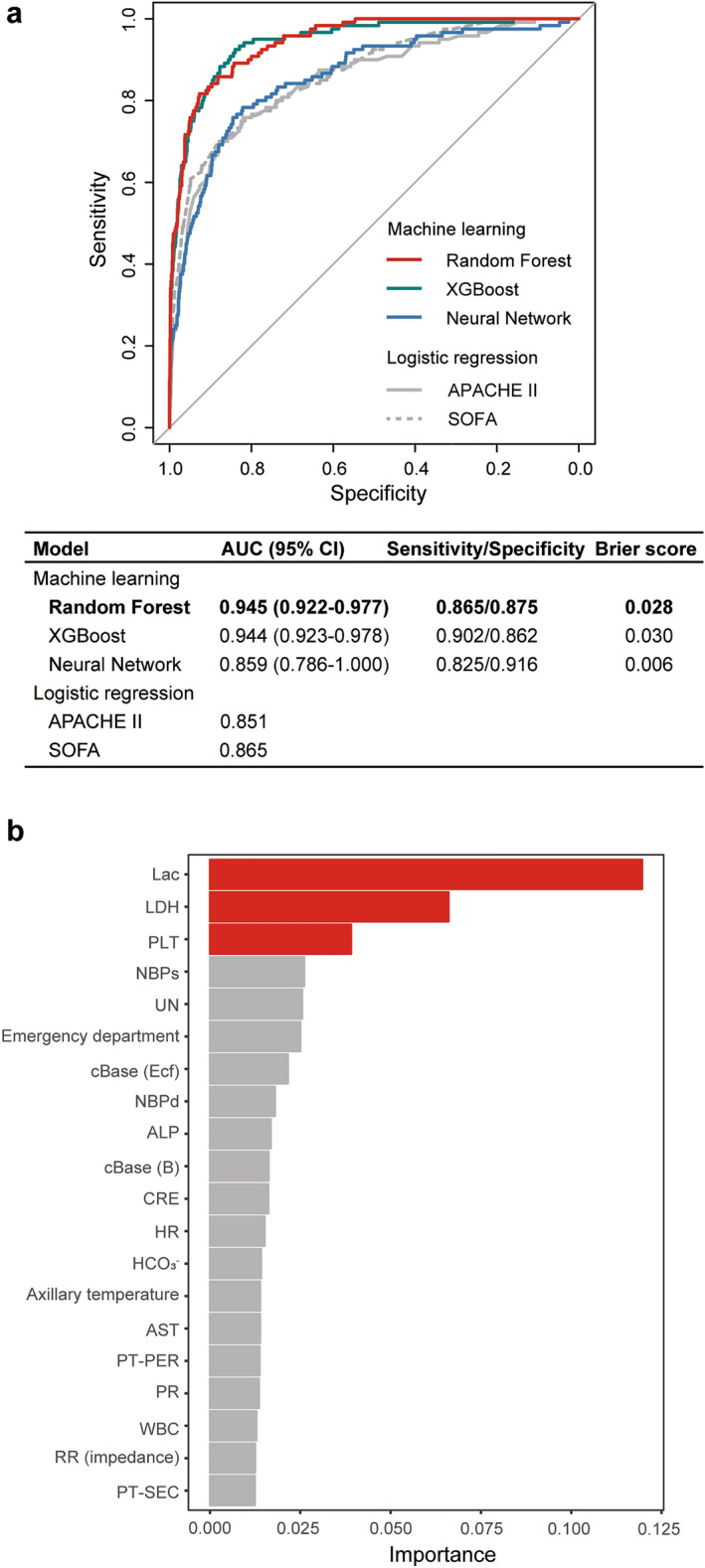
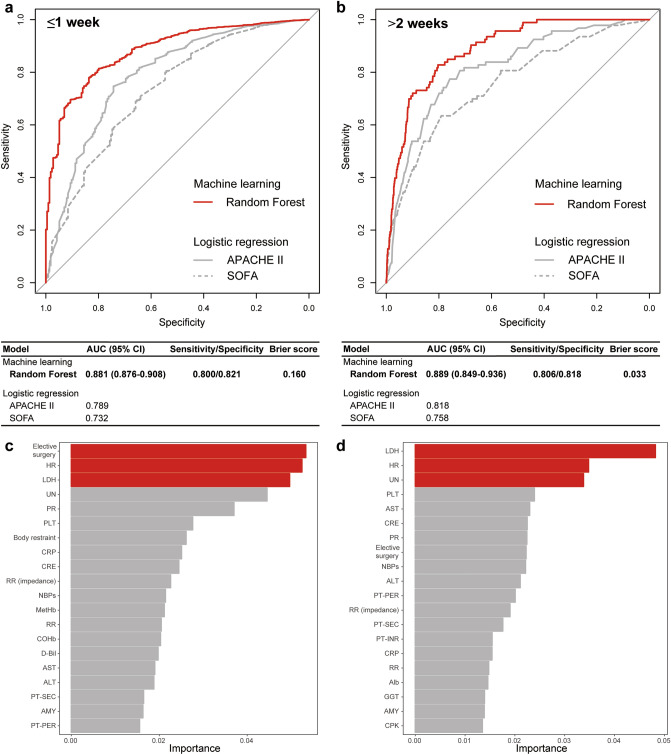
Machine learning can predict outcomes and determine variables contributing to precise prediction, and can thus classify patients with different risk factors of outcomes. This study aimed to investigate the predictive accuracy for mortality and length of stay in intensive care unit (ICU) patients using machine learning, and to identify the variables contributing to the precise prediction or classification of patients. Patients (n = 12,747) admitted to the ICU at Chiba University Hospital were randomly assigned to the training and test cohorts. After learning using the variables on admission in the training cohort, the area under the curve (AUC) was analyzed in the test cohort to evaluate the predictive accuracy of the supervised machine learning classifiers, including random forest (RF) for outcomes (primary outcome, mortality; secondary outcome, length of ICU stay). The rank of the variables that contributed to the machine learning prediction was confirmed, and cluster analysis of the patients with risk factors of mortality was performed to identify the important variables associated with patient outcomes. Machine learning using RF revealed a high predictive value for mortality, with an AUC of 0.945 (95% confidence interval [CI] 0.922-0.977). In addition, RF showed high predictive value for short and long ICU stays, with AUCs of 0.881 (95% CI 0.876-0.908) and 0.889 (95% CI 0.849-0.936), respectively. Lactate dehydrogenase (LDH) was identified as a variable contributing to the precise prediction in machine learning for both mortality and length of ICU stay. LDH was also identified as a contributing variable to classify patients into sub-populations based on different risk factors of mortality. The machine learning algorithm could predict mortality and length of stay in ICU patients with high accuracy. LDH was identified as a contributing variable in mortality and length of ICU stay prediction and could be used to classify patients based on mortality risk.
© 2022. The Author(s).
Conflict of interest statement
The authors declare no competing interests.
Figures

References
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
