

Minimally-Invasive Assisted Robotic Spine Surgery (MARSS)
- PMID: 35903260
- PMCID: PMC9316616
- DOI: 10.3389/fsurg.2022.884247
Minimally-Invasive Assisted Robotic Spine Surgery (MARSS)
Abstract
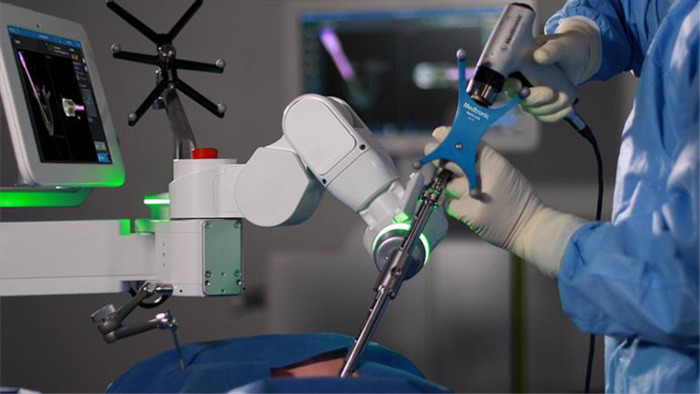
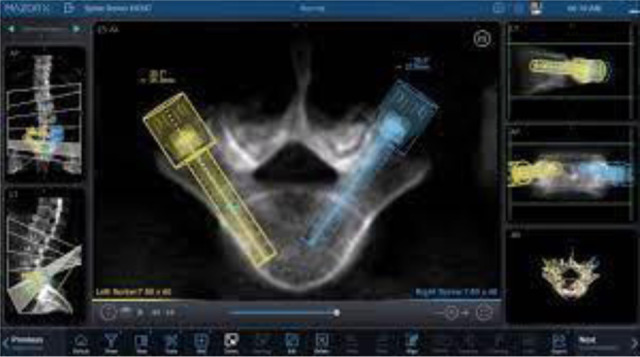
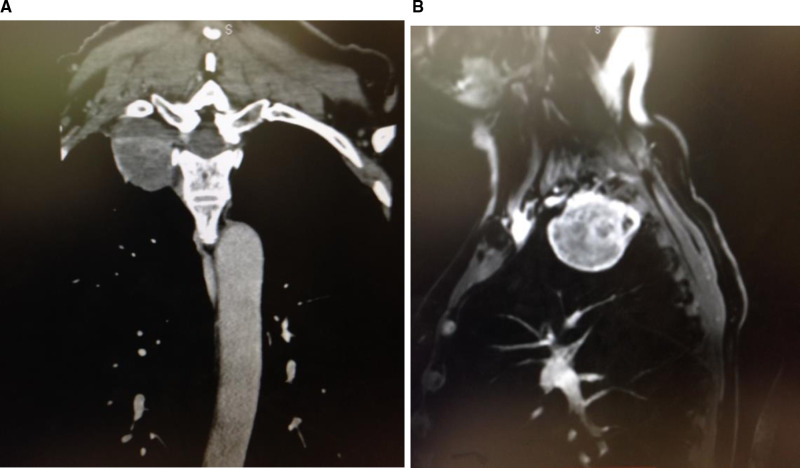
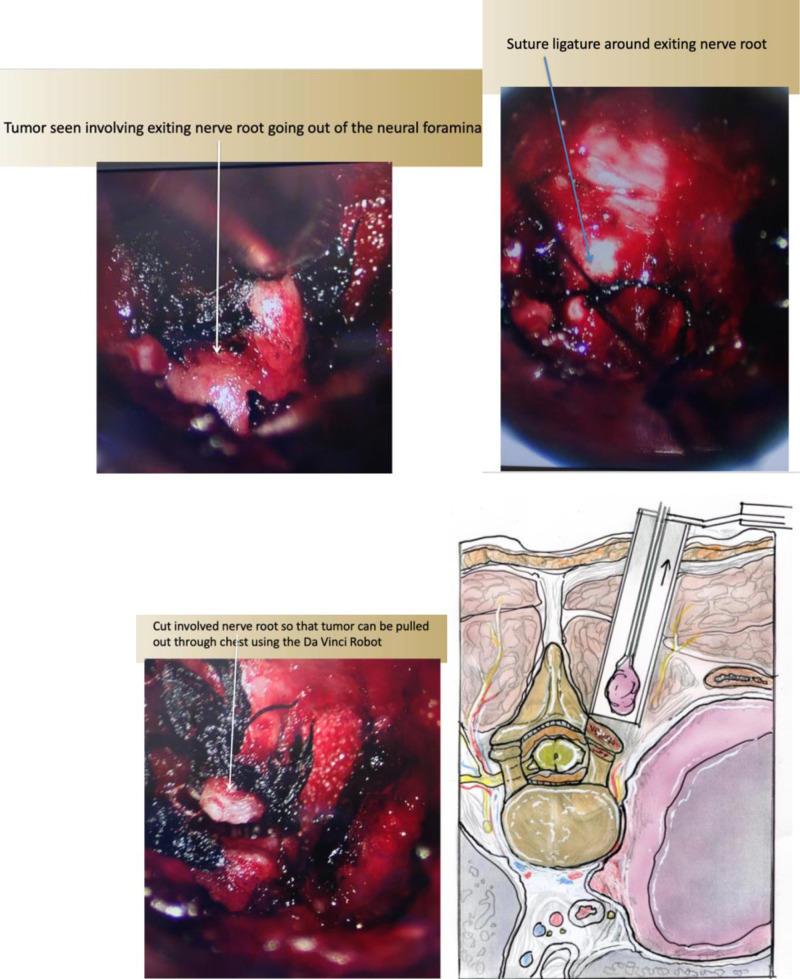
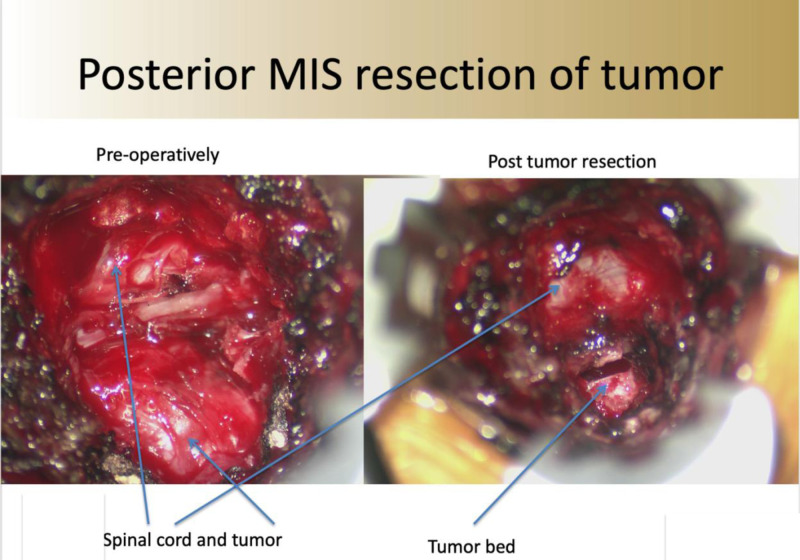
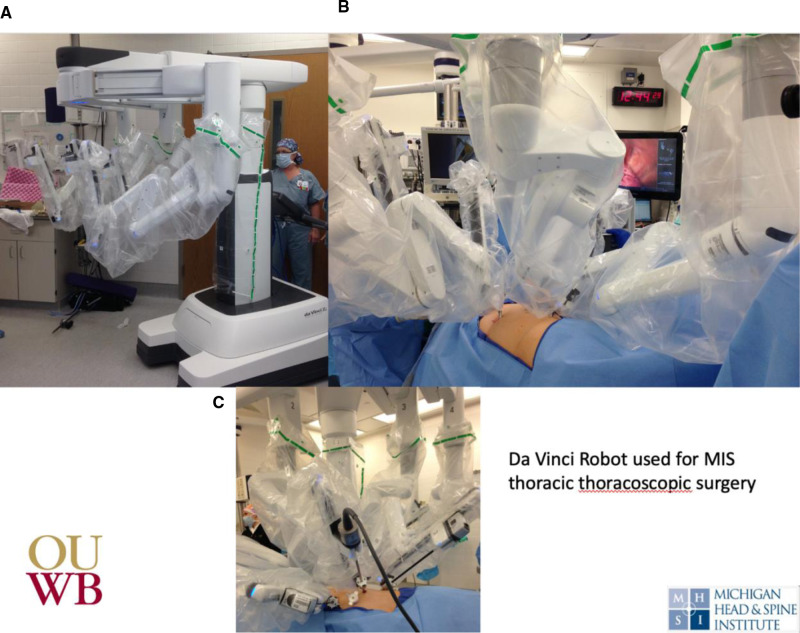
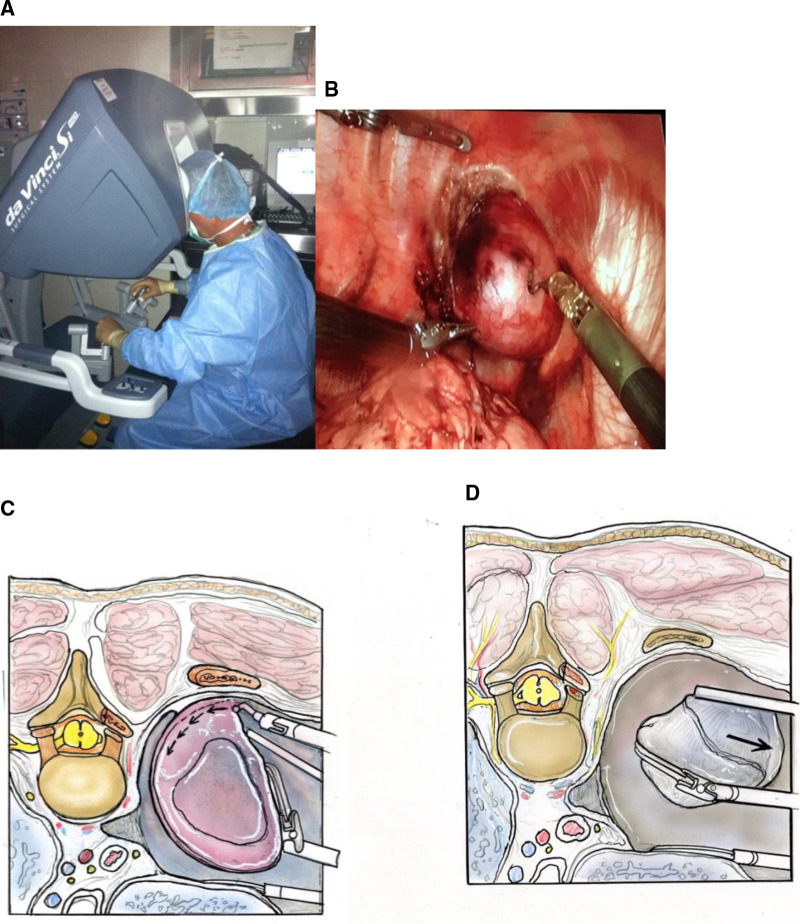
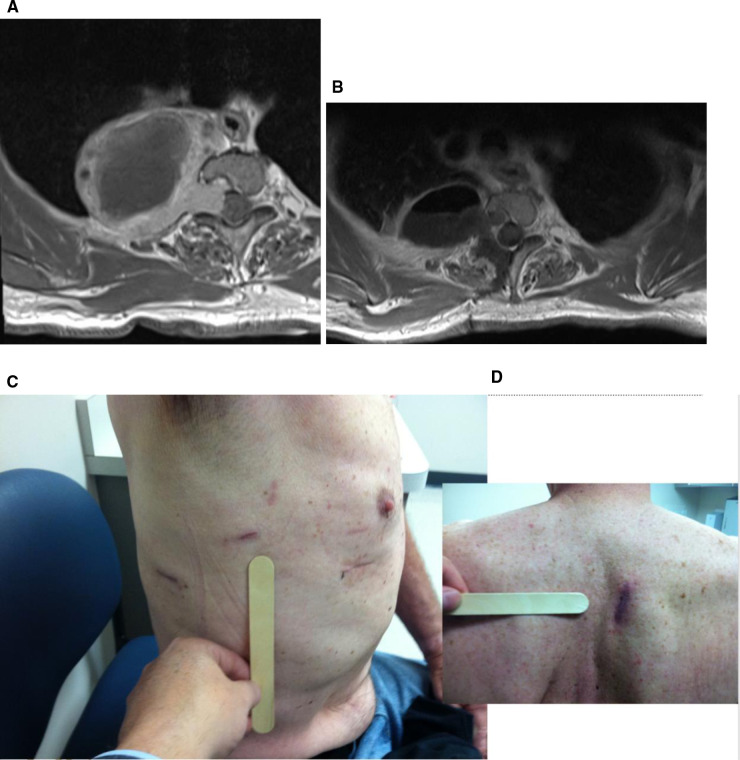
Minimally-Invasive robotic spine surgery (MARSS) has expanded the surgeons armamentarium to treat a variety of spinal disorders. In the last decade, robotic developments in spine surgery have improved the safety, accuracy and efficacy of instrumentation placement. Additionally, robotic instruments have been applied to remove tumors in difficult locations while maintaining minimally invasive access. Gross movements by the surgeon are translated into fine, precise movements by the robot. This is exemplified in this chapter with the use of the da Vinci robot to remove apical thoracic tumors. In this chapter, we will review the development, technological advancements, and cases that have been conducted using MARSS to treat spine pathology in a minimally invasive fashion.
Keywords: da Vinci; mazor X; minimally invasive spine surgery (MISS); minimally-invasive robotic spine surgery (MARSS); robotic; stereotactic transformation.
Copyright © 2022 Pérez de la Torre, Ramanathan, Williams and Perez-Cruet.
Figures



References
Publication types
LinkOut - more resources
Full Text Sources