

Deep sternal wound infection and pectoralis major muscle flap reconstruction: A single-center 20-year retrospective study
- PMID: 35903265
- PMCID: PMC9314736
- DOI: 10.3389/fsurg.2022.870044
Deep sternal wound infection and pectoralis major muscle flap reconstruction: A single-center 20-year retrospective study
Abstract
Background: One of the most drastic complications of median sternal incision is deep sternal wound infection (DSWI), as it can lead to prolonged hospitalization, increased expected costs, re-entry into the ICU and even reoperation. Since the pectoralis major muscle flap (PMMF) technique was proposed in the 1980s, it has been widely used for sternal reconstruction after debridement. Although numerous studies on DSWI have been conducted over the years, the literature on DSWI in Chinese population remains limited. The purpose of this study was to investigate the clinical characteristics of DSWI in patients and the clinical effect of the PMMF at our institution.
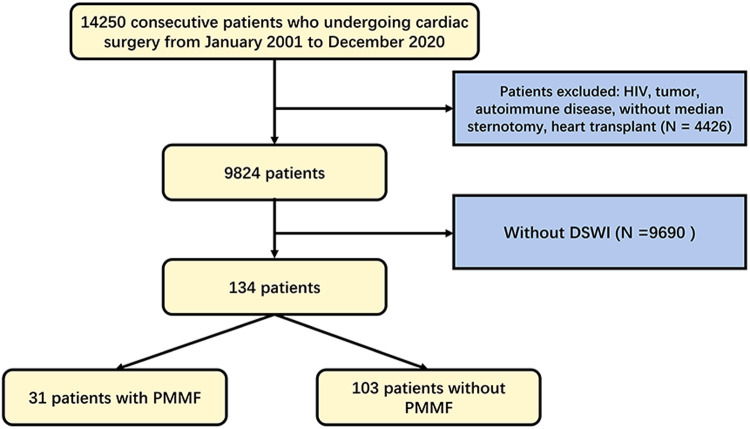
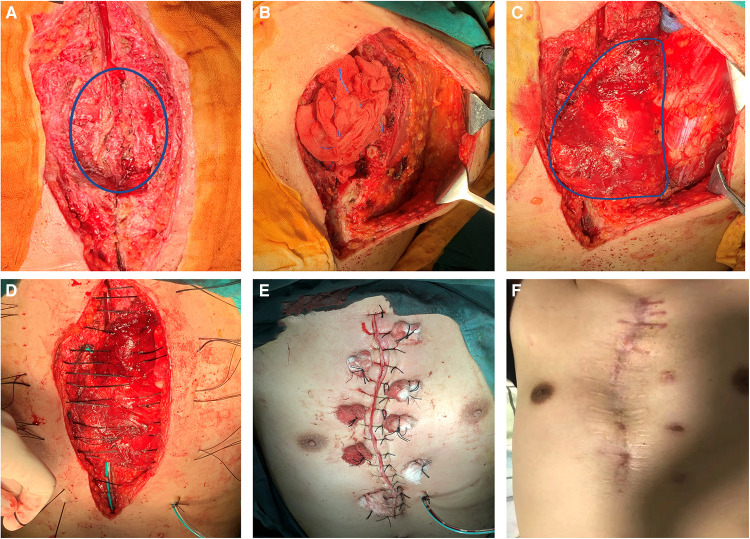
Methods: This study retrospectively analyzed all 14,250 consecutive patients who underwent cardiac surgery in the Department of Cardiothoracic Surgery of Drum Tower Hospital from 2001 to 2020. Ultimately, 134 patients were diagnosed with DSWI.,31 of whom had recently undergone radical debridement and transposition of the PMMF in the cardiothoracic surgery or burns and plastic surgery departments because of DSWIs, while the remaining patients had undergone conservative treatment or other methods of dressing debridement.
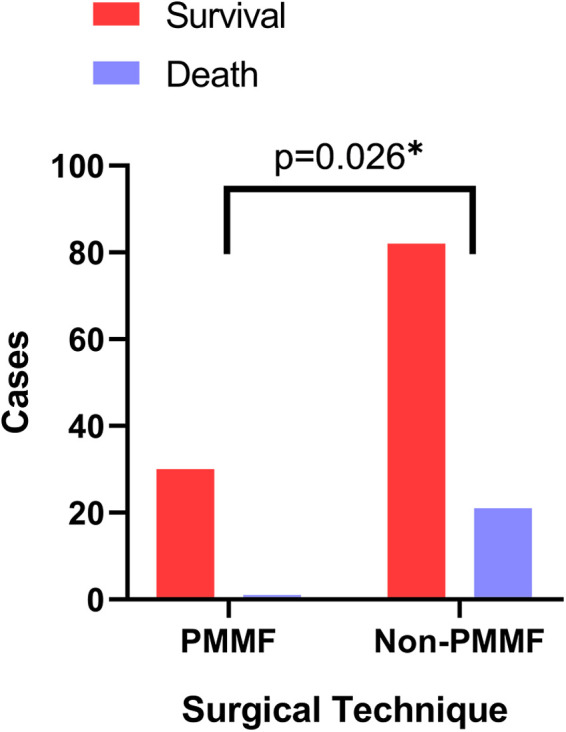
Results: In total, 9,824 patients were enrolled in the study between 2001 and 2020, of whom 134 met the DSWI criteria and 9690 served as controls. Body mass index (OR = 1.08; P = 0.02; 95% CI, 1.01∼1.16) and repeat sternotomy (OR = 5.93; P < 0.01; 95% CI, 2.88∼12.25) were important risk factors for DSWI. Of the 134 patients with DSWI, 31 underwent the PMMF technique, and the remaining 103 served as controls. There were significant differences in coronary artery bypass grafting (CABG) (P < 0.01), valve replacement (P = 0.04) and repeat sternotomy (P < 0.01) between the case group and the control group. The postoperative extubation time (P < 0.001), ICU time (P < 0.001), total hospitalization time (P < 0.001) and postoperative hospitalization time (P < 0.001) in the PMMF group were significantly lower than those in the control group. The results of multivariate regression analysis showed that PMMF surgery was an important protective factor for the postoperative survival of DSWI patients (OR = 0.12; P = 0.04; 95% CI, 0.01∼0.90).
Conclusions: Staphylococcus aureus was the most common bacteria causing DSWI, which was associated with BMI and reoperation, and can be validly treated with PMMF.
Keywords: DSWI; PMMF; cardiac surgery; flap; infection.
© 2022 Chen, Gao, Zhao, Ma, Su and Mo.
Conflict of interest statement
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Figures

Similar articles
-
Deep sternal wound infection after cardiac surgery in the Chinese population: a single-centre 15-year retrospective study.J Thorac Dis. 2017 Sep;9(9):3031-3037. doi: 10.21037/jtd.2017.08.41. J Thorac Dis. 2017. PMID: 29221276 Free PMC article.
-
[Analysis of surgical treatment with pectoralis major muscle flap for deep sternal infection after cardiac surgery: a case series of 189 patients].Zhonghua Wai Ke Za Zhi. 2015 Mar;53(3):193-6. Zhonghua Wai Ke Za Zhi. 2015. PMID: 26269014 Chinese.
-
Post-CABG Deep Sternal Wound Infection: A Retrospective Comparative Analysis of Early versus Late Referral to a Plastic Surgery Unit in a Tertiary Care Center.Indian J Plast Surg. 2021 Apr;54(2):157-162. doi: 10.1055/s-0041-1731256. Epub 2021 Jun 28. Indian J Plast Surg. 2021. PMID: 34239237 Free PMC article.
-
Prevention and management of deep sternal wound infection.Semin Thorac Cardiovasc Surg. 2004 Spring;16(1):62-9. doi: 10.1053/j.semtcvs.2004.01.005. Semin Thorac Cardiovasc Surg. 2004. PMID: 15366689 Review.
-
Association between HbA1c and deep sternal wound infection after coronary artery bypass: a systematic review and meta-analysis.J Cardiothorac Surg. 2024 Feb 4;19(1):51. doi: 10.1186/s13019-024-02549-6. J Cardiothorac Surg. 2024. PMID: 38311780 Free PMC article.
Cited by
-
Immediate flap increases patient safety for deep sternal wound infection: A meta-analysis.Int Wound J. 2023 Oct;20(8):3271-3278. doi: 10.1111/iwj.14207. Epub 2023 May 13. Int Wound J. 2023. PMID: 37178031 Free PMC article.
-
Risk factors for sternal wound infection after median sternotomy: A nested case-control study and time-to-event analysis.Int Wound J. 2024 Jul;21(7):e14965. doi: 10.1111/iwj.14965. Int Wound J. 2024. PMID: 38994878 Free PMC article.
-
A study on the preoperative risk factors for primary healing failure in the reconstruction of deep sternal wound infection with platelet-rich plasma and negative pressure trauma therapy.Int Wound J. 2023 Nov;20(9):3457-3466. doi: 10.1111/iwj.14216. Epub 2023 Jun 3. Int Wound J. 2023. PMID: 37269235 Free PMC article.
References
LinkOut - more resources
Full Text Sources
Miscellaneous