

Pediatric Metastatic Pheochromocytoma and Paraganglioma: Clinical Presentation and Diagnosis, Genetics, and Therapeutic Approaches
- PMID: 35903274
- PMCID: PMC9314859
- DOI: 10.3389/fendo.2022.936178
Pediatric Metastatic Pheochromocytoma and Paraganglioma: Clinical Presentation and Diagnosis, Genetics, and Therapeutic Approaches
Abstract
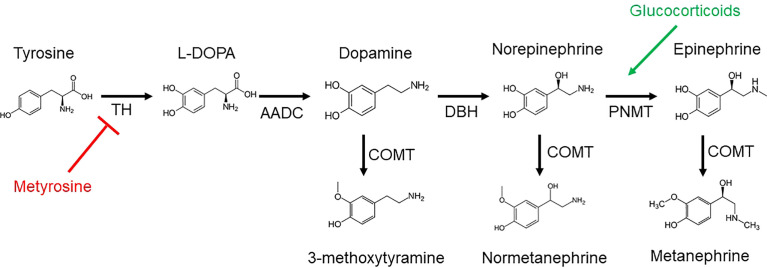
Although pediatric pheochromocytomas and paragangliomas (PPGLs) are rare, they have important differences compared to those in adults. Unfortunately, without timely diagnosis and management, these tumors have a potentially devastating impact on pediatric patients. Pediatric PPGLs are more often extra-adrenal, multifocal/metastatic, and recurrent, likely due to these tumors being more commonly due to a genetic predisposition than in adults. This genetic risk results in disease manifestations at an earlier age giving these tumors time to advance before detection. In spite of these problematic features, advances in the molecular and biochemical characterization of PPGLs have heralded an age of increasingly personalized medicine. An understanding of the genetic basis for an individual patient's tumor provides insight into its natural history and can guide clinicians in management of this challenging disease. In pediatric PPGLs, mutations in genes related to pseudohypoxia are most commonly seen, including the von Hippel-Lindau gene (VHL) and succinate dehydrogenase subunit (SDHx) genes, with the highest risk for metastatic disease associated with variants in SDHB and SDHA. Such pathogenic variants are associated with a noradrenergic biochemical phenotype with resultant sustained catecholamine release and therefore persistent symptoms. This is in contrast to paroxysmal symptoms (e.g., episodic hypertension, palpitations, and diaphoresis/flushing) as seen in the adrenergic, or epinephrine-predominant, biochemical phenotype (due to episodic catecholamine release) that is commonly observed in adults. Additionally, PPGLs in children more often present with signs and symptoms of catecholamine excess. Therefore, children, adolescents, and young adults present differently from older adults (e.g., the prototypical presentation of palpitations, perspiration, and pounding headaches in the setting of an isolated adrenal mass). These presentations are a direct result of genetic determinants and highlight the need for pediatricians to recognize these differences in order to expedite appropriate evaluations, including genetic testing. Identification and familiarity with causative genes inform surveillance and treatment strategies to improve outcomes in pediatric patients with PPGL.
Keywords: clinical presentation; diagnosis; genetics; metastatic; paraganglioma; pediatric; pheochromocytoma; therapeutic approach.
Copyright © 2022 Kuo, Nazari, Jha and Pacak.
Conflict of interest statement
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Figures
Similar articles
-
Semiquantitative 123I-Metaiodobenzylguanidine Scintigraphy to Distinguish Pheochromocytoma and Paraganglioma from Physiologic Adrenal Uptake and Its Correlation with Genotype-Dependent Expression of Catecholamine Transporters.J Nucl Med. 2015 Jun;56(6):839-46. doi: 10.2967/jnumed.115.154815. Epub 2015 Apr 16. J Nucl Med. 2015. PMID: 25883126
-
Pheochromocytoma and paraganglioma-an update on diagnosis, evaluation, and management.Pediatr Nephrol. 2020 Apr;35(4):581-594. doi: 10.1007/s00467-018-4181-2. Epub 2019 Jan 2. Pediatr Nephrol. 2020. PMID: 30603807 Review.
-
Pheochromocytoma and paraganglioma in children and adolescents.Acta Biochim Pol. 2023 Sep 17;70(3):487-493. doi: 10.18388/abp.2020_6955. Acta Biochim Pol. 2023. PMID: 37717273
-
Metastatic Pheochromocytoma and Paraganglioma: Somatostatin Receptor 2 Expression, Genetics, and Therapeutic Responses.J Clin Endocrinol Metab. 2023 Sep 18;108(10):2676-2685. doi: 10.1210/clinem/dgad166. J Clin Endocrinol Metab. 2023. PMID: 36946182 Free PMC article.
-
Supportive management of patients with pheochromocytoma/paraganglioma undergoing noninvasive treatment.Curr Opin Endocrinol Diabetes Obes. 2022 Jun 1;29(3):294-301. doi: 10.1097/MED.0000000000000724. Curr Opin Endocrinol Diabetes Obes. 2022. PMID: 35621181 Free PMC article. Review.
Cited by
-
Clinical utility of nuclear imaging in the evaluation of pediatric adrenal neoplasms.Front Oncol. 2023 Jan 17;12:1081783. doi: 10.3389/fonc.2022.1081783. eCollection 2022. Front Oncol. 2023. PMID: 36733351 Free PMC article. Review.
-
Multiple Primary Paragangliomas in a Pediatric Patient With von Hippel Lindau: A Diagnostic Dilemma.JCEM Case Rep. 2024 Sep 9;2(9):luae160. doi: 10.1210/jcemcr/luae160. eCollection 2024 Sep. JCEM Case Rep. 2024. PMID: 39253568 Free PMC article.
-
Current Strategies for Managing Pheochromocytoma and Paraganglioma in Children and Adolescents.Med Sci Monit. 2025 Apr 3;31:e947277. doi: 10.12659/MSM.947277. Med Sci Monit. 2025. PMID: 40176333 Free PMC article. Review.
-
Perioperative Blood Pressure Management Recommendations in Pediatric Pheochromocytoma: A 10-Year Narrative Review.Kidney Blood Press Res. 2025;50(1):61-82. doi: 10.1159/000542897. Epub 2024 Dec 3. Kidney Blood Press Res. 2025. PMID: 39626645 Free PMC article. Review.
-
The use of temozolomide in paediatric metastatic phaeochromocytoma/paraganglioma: A case report and literature review.Front Endocrinol (Lausanne). 2022 Nov 9;13:1066208. doi: 10.3389/fendo.2022.1066208. eCollection 2022. Front Endocrinol (Lausanne). 2022. PMID: 36440187 Free PMC article. Review.
References
-
- Lenders JWM, Kerstens MN, Amar L, Prejbisz A, Robledo M, Taieb D, et al. . Genetics, Diagnosis, Management and Future Directions of Research of Phaeochromocytoma and Paraganglioma: A Position Statement and Consensus of the Working Group on Endocrine Hypertension of the European Society of Hypertension. J Hypertens (2020) 38(8):1443–56. doi: 10.1097/HJH.0000000000002438 - DOI - PMC - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous