

Prevalence of Bertolotti's Syndrome in Lumbosacral Surgery Procedures
- PMID: 35903576
- PMCID: PMC9318490
- DOI: 10.7759/cureus.26341
Prevalence of Bertolotti's Syndrome in Lumbosacral Surgery Procedures
Abstract
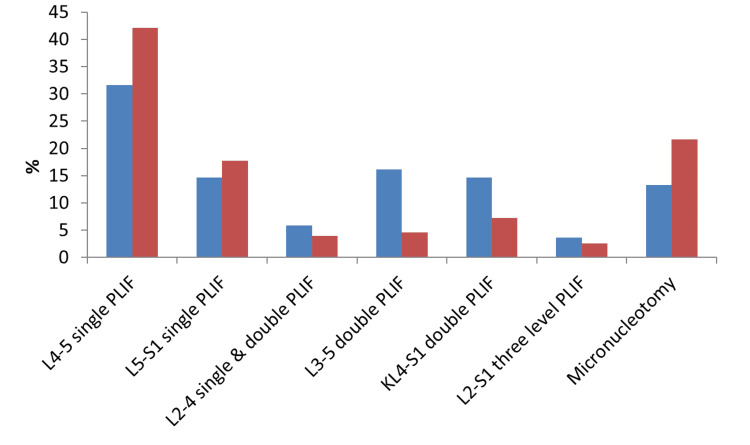
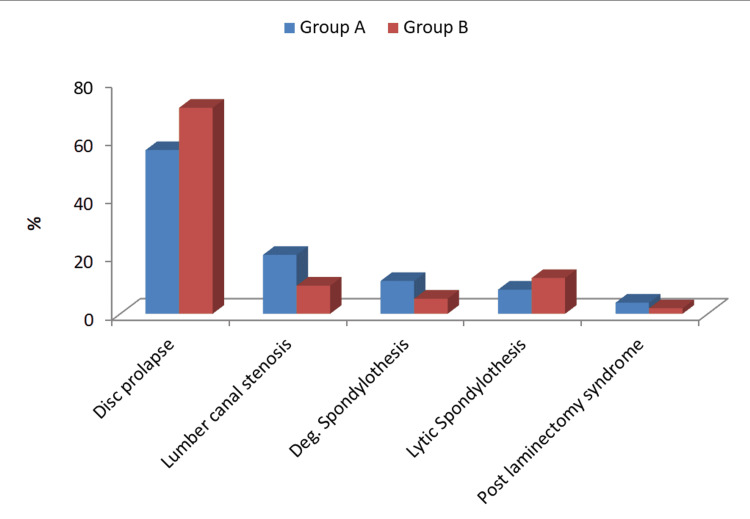
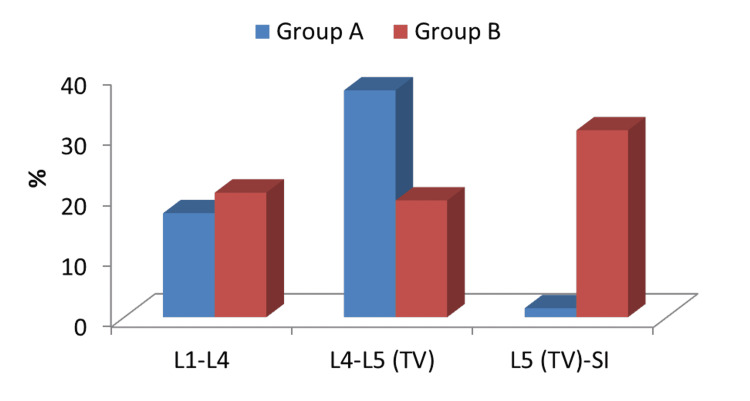
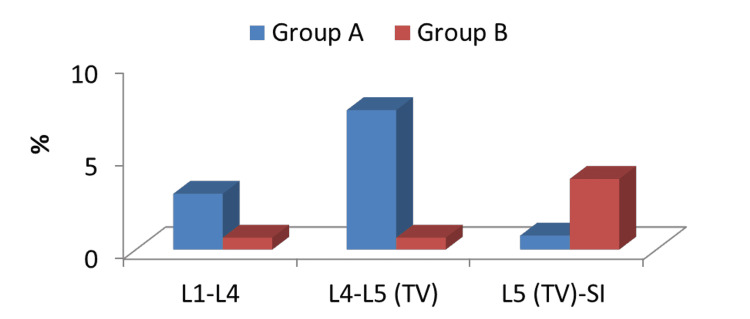
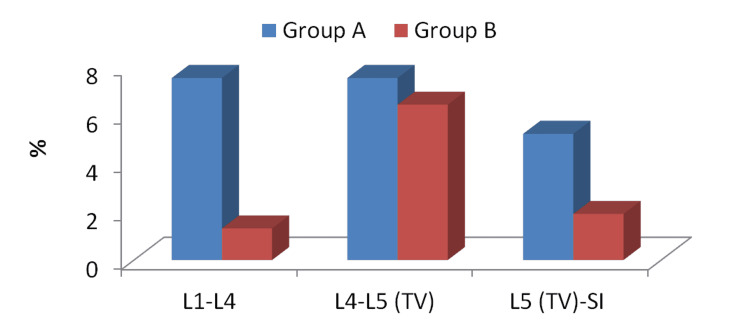
Introduction Bertolotti's syndrome (BS) describes the relationship between low back pain (LBP) and lumbosacral transitional vertebra (LSTV). It is a factor that is sometimes overlooked when it comes to evaluating and treating LBP.Because of the different diagnostic modalities and criteria used in the research, the LSTV incidence in the general population varies greatly, and hence the link between LSTV and LBP remains contentious. Some researchers found no link between low back pain and LSTV. As a result, the management of BS remains controversial and multiple treatments have been suggested, including locally injected steroid and various surgical approaches. Methods This retrospective cohort study included a total of 288 patients who underwent lumbosacral surgical procedures for disc prolapse, lumbar canal stenosis, spondylolithesis and post-laminectomy syndrome during the period between January 2016 and May 2020. Trauma, tumours and scoliotic patients were excluded. All data were collected from the departmental database. All cases were done by the same surgical team at El Hadra University Hospital Spine Unit, Egypt. The patients were divided into two groups. Group A consisted of 133 patients in whom LSTV was detected by radiologic findings. In contrast, Group B consisted of 155 patients in whom LSTV was not detected. Results In our study, the overall prevalence of LSTV among 288 patients who underwent lumbosacral surgical interventions was 46.2%. On comparing the incidence of surgical interventions between both groups, there was non-significant difference in most of surgical interventions. The incidence of L3-5 double-level posterior lumbar interbody fusion (PLIF) among LSTV patients was 16.5% compared to 4.61% in the other group. The incidence of L4-S1 double-level PLIF among LSTV patients was 15.04% compared to 7.24% in the other group. Regarding adjacent segment pathology, the incidence of lumbar canal stenosis and degenerative spondylolithesis was higher in the LSTV group (20.3% and 11.3%, respectively) compared to the non-LSTV group (9.7% and 5.2%, respectively). The incidence of disc prolapse was lower in the LSTV group (56.39%) compared to the non-LSTV group (71.0%). There was a non-significant difference between the incidence of lytic spondylolithesis and postlaminectomy syndrome between both groups. Conclusion The overall prevalence of LSTV among all cases who underwent lumbosacral surgical procedures at the El Hadra University Hospital was 46.2%. The incidence of lumbar canal stenosis and degenerative spondylolithesis was higher in the LSTV group compared to the non-LSTV group. However, the incidence of disc prolapse was lower in the LSTV group compared to the non-LSTV group. The incidence of disc prolapse and degenerative spondylolithesis at the L4-5 level was higher in the LSTV group compared to the non-LSTV group. In contrast, the incidence at L5-S1 was lower in the LSTV group compared to the non-LSTV group. Hence, LSTV is considered a risk factor for disc degenerative changes at the level above the transitional vertebra level.
Keywords: bertolotti’s syndrome; degeneration; lstv; lumbosacral surgery; micronucleotomy; plif.
Copyright © 2022, Ashour et al.
Conflict of interest statement
The authors have declared that no competing interests exist.
Figures
Similar articles
-
An update on the prevalence and management of Bertolotti's syndrome.Front Surg. 2024 Dec 12;11:1486811. doi: 10.3389/fsurg.2024.1486811. eCollection 2024. Front Surg. 2024. PMID: 39726766 Free PMC article. Review.
-
Minimally invasive tubular resection of the anomalous transverse process in patients with Bertolotti's syndrome: presented at the 2013 Joint Spine Section Meeting: clinical article.J Neurosurg Spine. 2014 Mar;20(3):283-90. doi: 10.3171/2013.11.SPINE13132. Epub 2013 Dec 20. J Neurosurg Spine. 2014. PMID: 24358999
-
Surgical Treatment of a Rare Presentation of Bertolotti's Syndrome from Castellvi Type IV Lumbosacral Transitional Vertebra: Case Report and Review of the Literature.J Neurol Surg Rep. 2018 Jul;79(3):e70-e74. doi: 10.1055/s-0038-1667172. Epub 2018 Jul 30. J Neurol Surg Rep. 2018. PMID: 30083494 Free PMC article.
-
Development of a novel in vitro cadaveric model for analysis of biomechanics and surgical treatment of Bertolotti syndrome.Spine J. 2020 Apr;20(4):638-656. doi: 10.1016/j.spinee.2019.10.011. Epub 2019 Oct 25. Spine J. 2020. PMID: 31669612
-
Risks Associated with Surgical Management of Lumbosacral Transitional Vertebrae: Systematic Review of Surgical Considerations and Illustrative Case.World Neurosurg. 2024 Jun;186:e54-e64. doi: 10.1016/j.wneu.2024.02.033. Epub 2024 Feb 11. World Neurosurg. 2024. PMID: 38350597
Cited by
-
Functional outcomes of microdiscectomy in Bertolotti syndrome: the relationship between lumbosacral transitional vertebrae and lumbar disc herniation: a prospective study in Greece.Asian Spine J. 2025 Feb;19(1):94-101. doi: 10.31616/asj.2024.0213. Epub 2025 Feb 24. Asian Spine J. 2025. PMID: 40037323 Free PMC article.
-
An update on the prevalence and management of Bertolotti's syndrome.Front Surg. 2024 Dec 12;11:1486811. doi: 10.3389/fsurg.2024.1486811. eCollection 2024. Front Surg. 2024. PMID: 39726766 Free PMC article. Review.
References
-
- Contribution to the knowledge of the vices of regional differentiation of the spine with special regard to the assimilation of the fifth lumbar vertebrae into the sacrum. Bertolotti M. Radiologia Medica. 1917;4:113–144.
-
- Anomalous lumbosacral articulations and low-back pain. Evaluation and treatment. Jönsson B, Strömqvist B, Egund N. Spine (Phila Pa 1976) 1989;14:831–834. - PubMed
-
- Clinical significance of congenital lumbosacral malformations in young male population with prolonged low back pain. Taskaynatan MA, Izci Y, Ozgul A, Hazneci B, Dursun H, Kalyon TA. Spine (Phila Pa 1976) 2005;30:0–3. - PubMed
-
- Bertolotti's syndrome. A cause of back pain in young people. Quinlan JF, Duke D, Eustace S. J Bone Joint Surg Br. 2006;88:1183–1186. - PubMed
LinkOut - more resources
Full Text Sources
Research Materials
Miscellaneous