

Association of Cell Death Markers With Tumor Immune Cell Infiltrates After Chemo-Radiation in Cervical Cancer
- PMID: 35903697
- PMCID: PMC9316180
- DOI: 10.3389/fonc.2022.892813
Association of Cell Death Markers With Tumor Immune Cell Infiltrates After Chemo-Radiation in Cervical Cancer
Abstract
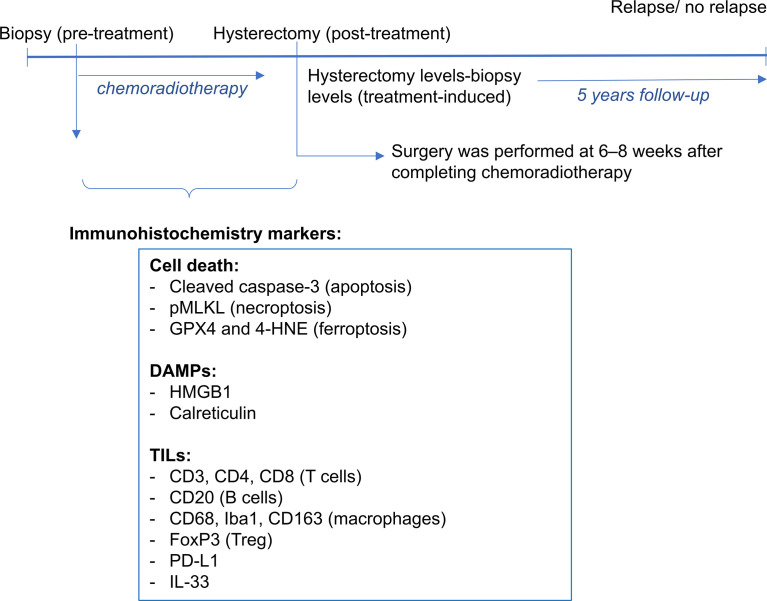
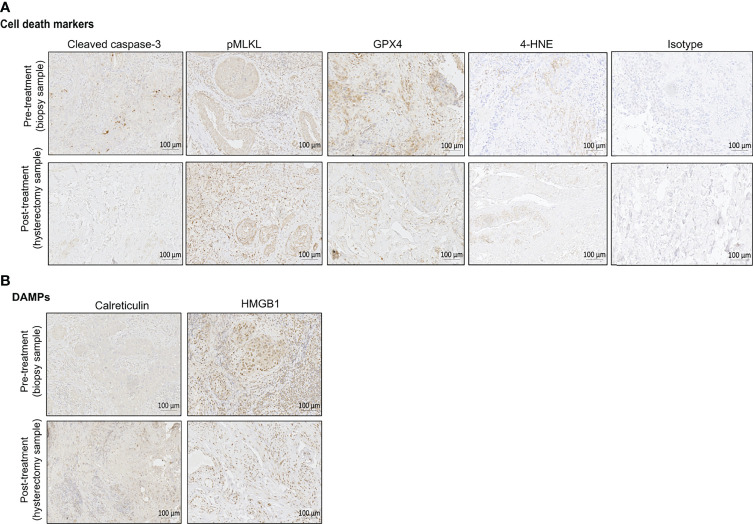
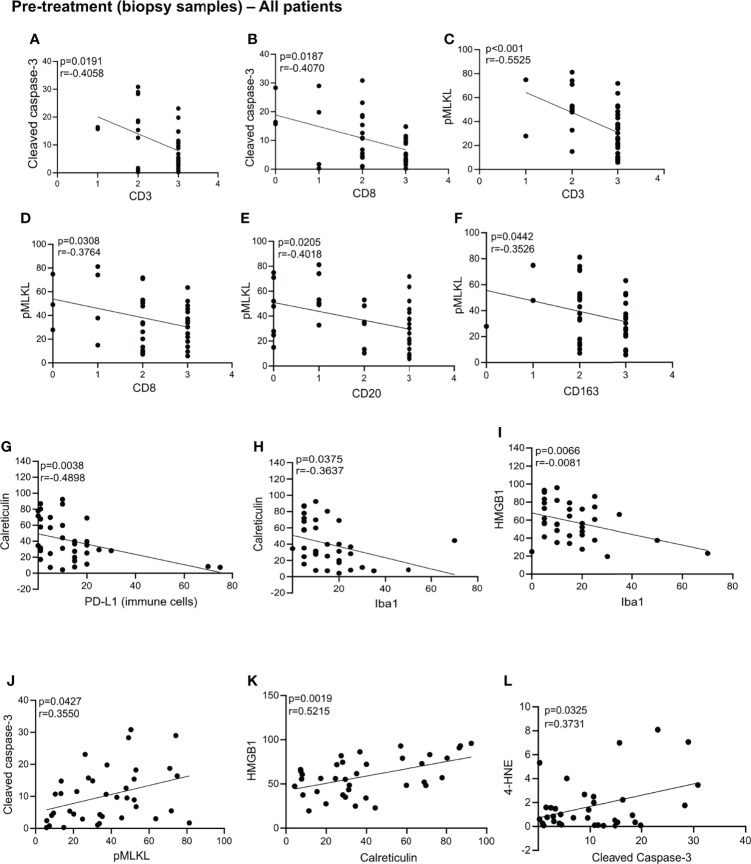
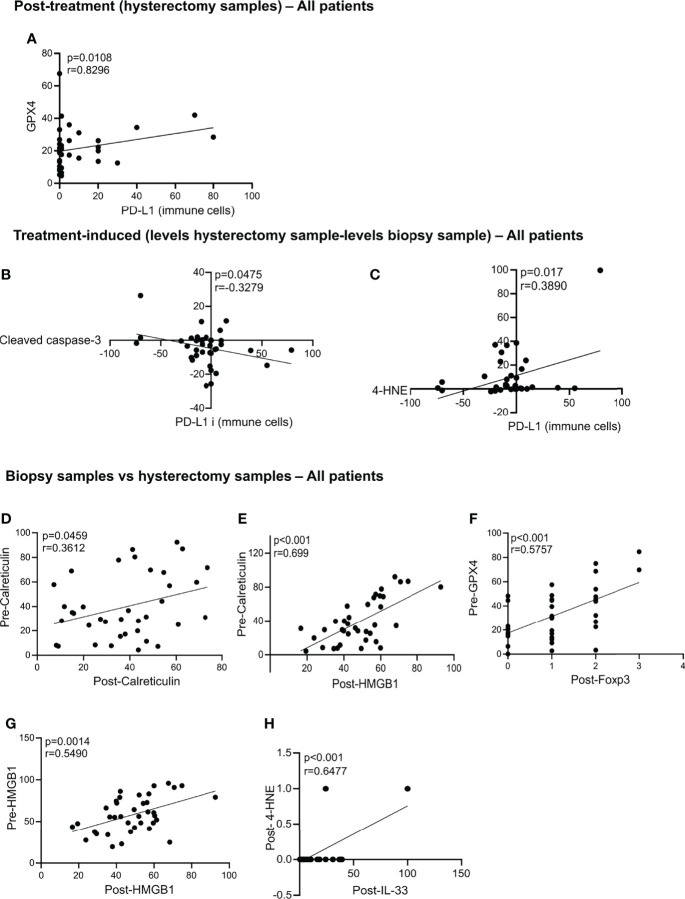
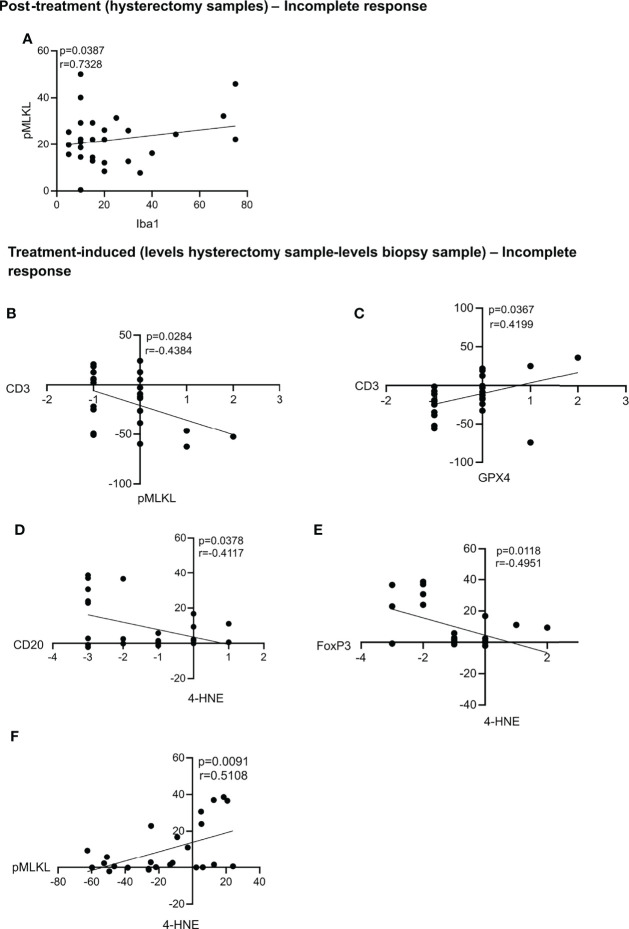
Irradiation induces distinct cellular responses such as apoptosis, necroptosis, iron-dependent cell death (a feature of ferroptosis), senescence, and mitotic catastrophe. Several of these outcomes are immunostimulatory and may represent a potential for immunogenic type of cell death (ICD) induced by radiotherapy triggering abscopal effects. The purpose of this study is to determine whether intra-tumoral ICD markers can serve as biomarkers for the prediction of patient's outcomes defined as the metastasis status and survival over a 5-year period. Thirty-eight patients with locally advanced cervical cancer, treated with neoadjuvant chemoradiotherapy using cisplatin were included in this study. Pre-treatment tumor biopsy and post-treatment hysterectomy samples were stained for cell death markers and danger associated molecular patterns (DAMPs): cleaved caspase-3 (apoptosis), phosphorylated mixed lineage kinase domain like pseudokinase (pMLKL; necroptosis), glutathione peroxidase 4 (GPX4; ferroptosis) and 4-hydroxy-2-noneal (4-HNE; ferroptosis), high mobility group box 1 (HMGB1) and calreticulin. Although these markers could not predict the patient's outcome in terms of relapse or survival, many significantly correlated with immune cell infiltration. For instance, inducing ferroptosis post-treatment seems to negatively impact immune cell recruitment. Measuring ICD markers could reflect the impact of treatment on the tumor microenvironment with regard to immune cell recruitment and infiltration.
One sentence summary: Cell death readouts during neoadjuvant chemoradiation in cervical cancer.
Keywords: biomarkers; cell death; cervical cancer; immunogenic cell death; tumor infiltrating leucocytes.
Copyright © 2022 Oltean, Lippens, Lemeire, De Tender, Vuylsteke, Denys, Vandecasteele, Vandenabeele and Adjemian.
Conflict of interest statement
Author MV was employed by Gnomixx. The remaining authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Figures
References
-
- Cibula D, Pötter R, Planchamp F, Avall-Lundqvist E, Fischerova D, Haie Meder C, et al. The European Society of Gynaecological Oncology/European Society for Radiotherapy and Oncology/European Society of Pathology Guidelines for the Management of Patients With Cervical Cancer. Int J Gynecol Cancer (2018) 28:641–55. doi: 10.1097/IGC.0000000000001216 - DOI - PubMed
-
- Couvreur K, Naert E, De Jaeghere E, Tummers P, Makar A, De Visschere P, et al. Neo-Adjuvant Treatment of Adenocarcinoma and Squamous Cell Carcinoma of the Cervix Results in Significantly Different Pathological Complete Response Rates. BMC Cancer (2018) 18:1–10. doi: 10.1186/s12885-018-5007-0 - DOI - PMC - PubMed
LinkOut - more resources
Full Text Sources
Research Materials