

Diabetic Striatopathy Complicated With Acute Ischemic Stroke: A Case Report
- PMID: 35903807
- PMCID: PMC9315246
- DOI: 10.3389/fnins.2022.877479
Diabetic Striatopathy Complicated With Acute Ischemic Stroke: A Case Report
Abstract
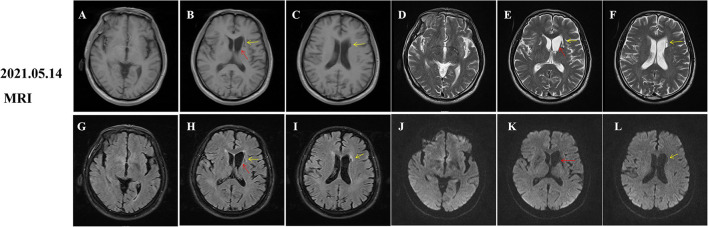
Diabetic striatopathy (DS) is a rare complication secondary to hyperglycemia, featured by the choreiform movements and reversible striatal abnormalities on neuroimaging. Several studies have described the clinical characteristics of DS, however, the simultaneous occurrence of DS and acute ischemic stroke (AIS) in the striatum has not been reported. Herein, we report a 68-year-old man with uncontrolled type 2 diabetes who experienced the progressive involuntary movement of the right upper and lower limbs for 10 days. We initially considered this patient as an AIS with hemorrhage in the left basal ganglia and adjacent area because his brain magnetic resonance imaging (MRI) showed hyperintensity on fluid-attenuated inversion recovery (FLAIR) and diffusion-weighted imaging (DWI) images, as well as slight T1-hyperintensity around T1-hypointensity. However, his symptoms worsen persistently, which was inconsistent with neuroimaging findings. Further computed tomography (CT) scan revealed an extensive hyper-density and focal low-density in the left striatum, suggesting the diagnosis of DS and AIS. His symptoms were in complete remission after 2 months of glucose control. However, striatal hyperintensity on T1 images was significantly increased compared to the initial images, which disappeared 18 months later. Additionally, DWI hyperintensity on infarction lesions disappeared, while softening lesions and gliosis were observed on the follow-up MRI images. Therefore, we finally diagnosed the patient as DS complicated with AIS. This report highlights that DS and AIS could occur simultaneously in the striatum after hyperglycemia, which is easily misdiagnosed as AIS with hemorrhage and requires clinicians to pay more attention to avoid misdiagnosis and delayed treatment.
Keywords: acute ischemic stroke; chorea; diabetic striatopathy; hyperglycemia; involuntary movement.
Copyright © 2022 Huang, Qi, Li, Li and Yang.
Conflict of interest statement
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Figures


References
Publication types
LinkOut - more resources
Full Text Sources