

Identification of Distinct Subgroups in Moderately Severe Rheumatic Mitral Stenosis Using Data-Driven Phenotyping of Longitudinal Hemodynamic Progression
- PMID: 35904199
- PMCID: PMC9375495
- DOI: 10.1161/JAHA.121.026375
Identification of Distinct Subgroups in Moderately Severe Rheumatic Mitral Stenosis Using Data-Driven Phenotyping of Longitudinal Hemodynamic Progression
Abstract
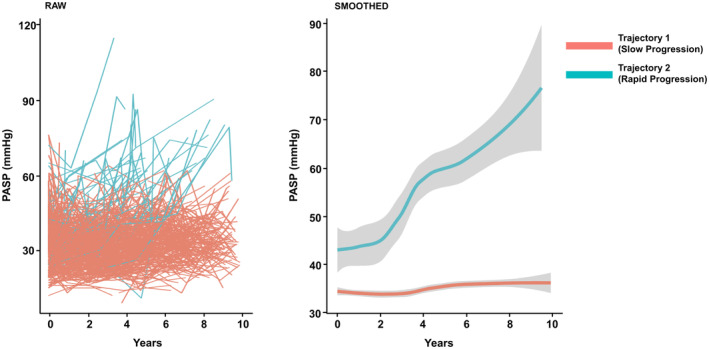
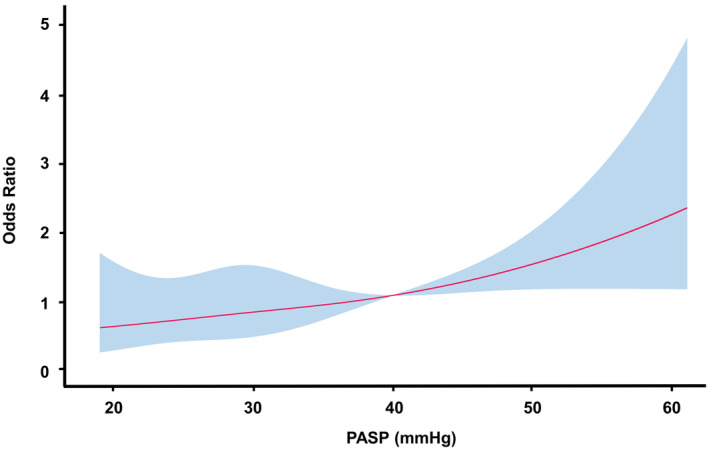
Background Rheumatic mitral stenosis is a significant cause of valvular heart disease. Pulmonary arterial systolic pressure (PASP) reflects the hemodynamic consequences of mitral stenosis and is used to determine treatment strategies. However, PASP progression and expected outcomes based on PASP changes in patients with moderately severe mitral stenosis remain unclear. Methods and Results A total of 436 patients with moderately severe rheumatic mitral stenosis (valve area 1.0-1.5 cm2) were enrolled. Composite outcomes included all-cause mortality and hospitalization for heart failure. Data-driven phenotyping identified 2 distinct trajectory groups based on PASP progression: rapid (8.7%) and slow (91.3%). Patients in the rapid progression group were older and had more diabetes and atrial fibrillation than those in the slow progression group (all P<0.05). The initial mean diastolic pressure gradient and PASP were higher in the rapid progression group than in the slow progression group (6.2±2.4 mm Hg versus 5.1±2.0 mm Hg [P=0.001] and 42.3±13.3 mm Hg versus 33.0±9.2 mm Hg [P<0.001], respectively). The rapid progression group had a poorer event-free survival rate than the slow progression group (log-rank P<0.001). Rapid PASP progression was a significant risk factor for composite outcomes even after adjusting for comorbidities (hazard ratio, 3.08 [95% CI, 1.68-5.64]; P<0.001). Multivariate regression analysis revealed that PASP >40 mm Hg was independently associated with allocation to the rapid progression group (odds ratio, 4.95 [95% CI, 2.08-11.99]; P<0.001). Conclusions Rapid PASP progression was associated with a higher risk of the composite outcomes. The main independent predictor for rapid progression group allocation was initial PASP >40 mm Hg.
Keywords: composite outcomes; data‐driven phenotyping; latent class trajectory modeling; pulmonary arterial systolic pressure; rheumatic mitral stenosis.
Figures


Similar articles
-
Prognostic Value of Pulmonary Artery Systolic Pressure in Severe Rheumatic Mitral Stenosis.Circ Cardiovasc Imaging. 2024 Oct;17(10):e016302. doi: 10.1161/CIRCIMAGING.123.016302. Epub 2024 Oct 15. Circ Cardiovasc Imaging. 2024. PMID: 39405388
-
Severe Rheumatic Mitral Stenosis, Worse Left Atrial Mechanics is Closely Associated with Echo Criteria for Intervention.J Cardiovasc Echogr. 2022 Jan-Mar;32(1):38-46. doi: 10.4103/jcecho.jcecho_80_21. Epub 2022 Apr 20. J Cardiovasc Echogr. 2022. PMID: 35669131 Free PMC article.
-
Differences in Characteristics, Left Atrial Reverse Remodeling, and Functional Outcomes after Mitral Valve Replacement in Patients with Low-Gradient Very Severe Mitral Stenosis.J Am Soc Echocardiogr. 2016 Aug;29(8):759-767. doi: 10.1016/j.echo.2016.03.012. Epub 2016 Apr 20. J Am Soc Echocardiogr. 2016. PMID: 27106010
-
Low-Gradient Severe Mitral Stenosis: Hemodynamic Profiles, Clinical Characteristics, and Outcomes.J Am Heart Assoc. 2019 Mar 5;8(5):e010736. doi: 10.1161/JAHA.118.010736. J Am Heart Assoc. 2019. PMID: 30793648 Free PMC article.
-
Pulmonary Hypertension in Transcatheter Mitral Valve Repair for Secondary Mitral Regurgitation: The COAPT Trial.J Am Coll Cardiol. 2020 Dec 1;76(22):2595-2606. doi: 10.1016/j.jacc.2020.09.609. J Am Coll Cardiol. 2020. PMID: 33243380 Clinical Trial.
Cited by
-
2023 Korean Society of Echocardiography position paper for the diagnosis and management of valvular heart disease, part II: mitral and tricuspid valve disease.J Cardiovasc Imaging. 2024 Jun 25;32(1):10. doi: 10.1186/s44348-024-00021-6. J Cardiovasc Imaging. 2024. PMID: 38951920 Free PMC article. Review.
References
-
- Marcus RH, Sareli P, Pocock WA, Barlow JB. The spectrum of severe rheumatic mitral valve disease in a developing country: correlations among clinical presentation, surgical pathologic findings, and hemodynamic sequelae. Ann Intern Med. 1994;120:177–183. doi: 10.7326/0003-4819-120-3-199402010-00001 - DOI - PubMed
-
- Otto CM, Nishimura RA, Bonow RO, Carabello BA, Erwin JP III, Gentile F, Jneid H, Krieger EV, Mack M, McLeod C. 2020 ACC/AHA guideline for the management of patients with valvular heart disease: a report of the American College of Cardiology/American Heart Association Joint Committee on Clinical Practice Guidelines. Circulation. 2021;143:e72–e227. doi: 10.1161/CIR.0000000000000923 - DOI - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
