

Resting energy expenditure in children at risk of hypothalamic dysfunction
- PMID: 35904233
- PMCID: PMC9346331
- DOI: 10.1530/EC-22-0276
Resting energy expenditure in children at risk of hypothalamic dysfunction
Abstract
Objective: Children with suprasellar brain damage are at risk of hypothalamic dysfunction (HD). HD may lead to decreased resting energy expenditure (REE). Decreased REE, however, is not present in all children with HD. Our aim was to assess which children suspect for HD have low REE, and its association with clinical severity of HD or radiological hypothalamic damage.
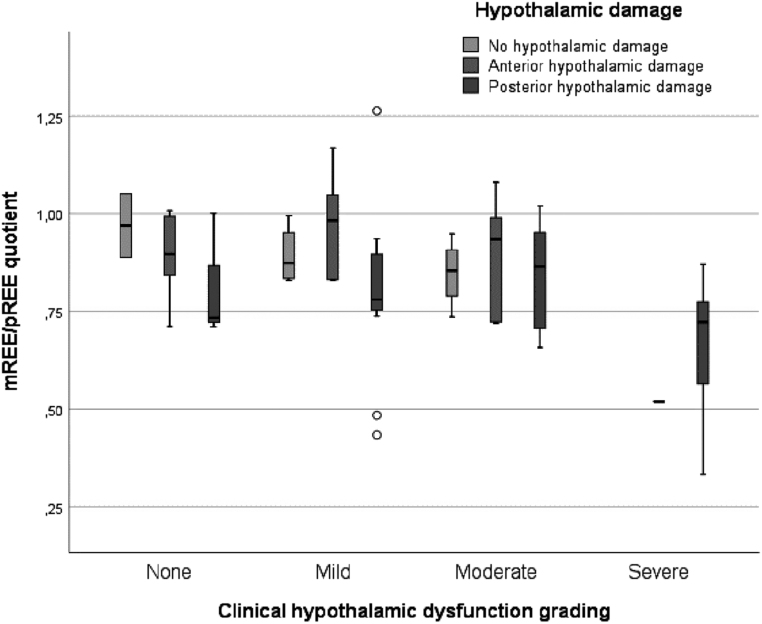
Patients and methods: A retrospective cohort study was performed. Measured REE (mREE) of children at risk of HD was compared to predicted REE (pREE). Low REE was defined as mREE <90% of predicted. The mREE/pREE quotient was associated to a clinical score for HD symptoms and to radiological hypothalamic damage.
Results: In total, 67 children at risk of HD (96% brain tumor diagnosis) with a mean BMI SDS of +2.3 ± 1.0 were included. Of these, 45 (67.2%) had low mREE. Children with severe HD had a significant lower mean mREE/pREE quotient compared to children with no, mild, or moderate HD. Mean mREE/pREE quotient of children with posterior hypothalamic damage was significantly lower compared to children with no or anterior damage. Tumor progression or tumor recurrence, severe clinical HD, and panhypopituitarism with diabetes insipidus (DI) were significant risk factors for reduced REE.
Conclusion: REE may be lowered in children with hypothalamic damage and is associated to the degree of clinical HD. REE is, however, not lowered in all children suspect for HD. For children with mild or moderate clinical HD symptoms, REE measurements may be useful to distinguish between those who may benefit from obesity treatment that increases REE from those who would be better helped using other obesity interventions.
Keywords: hypothalamic obesity; posterior hypothalamic damage; resting energy expenditure; suprasellar tumor.
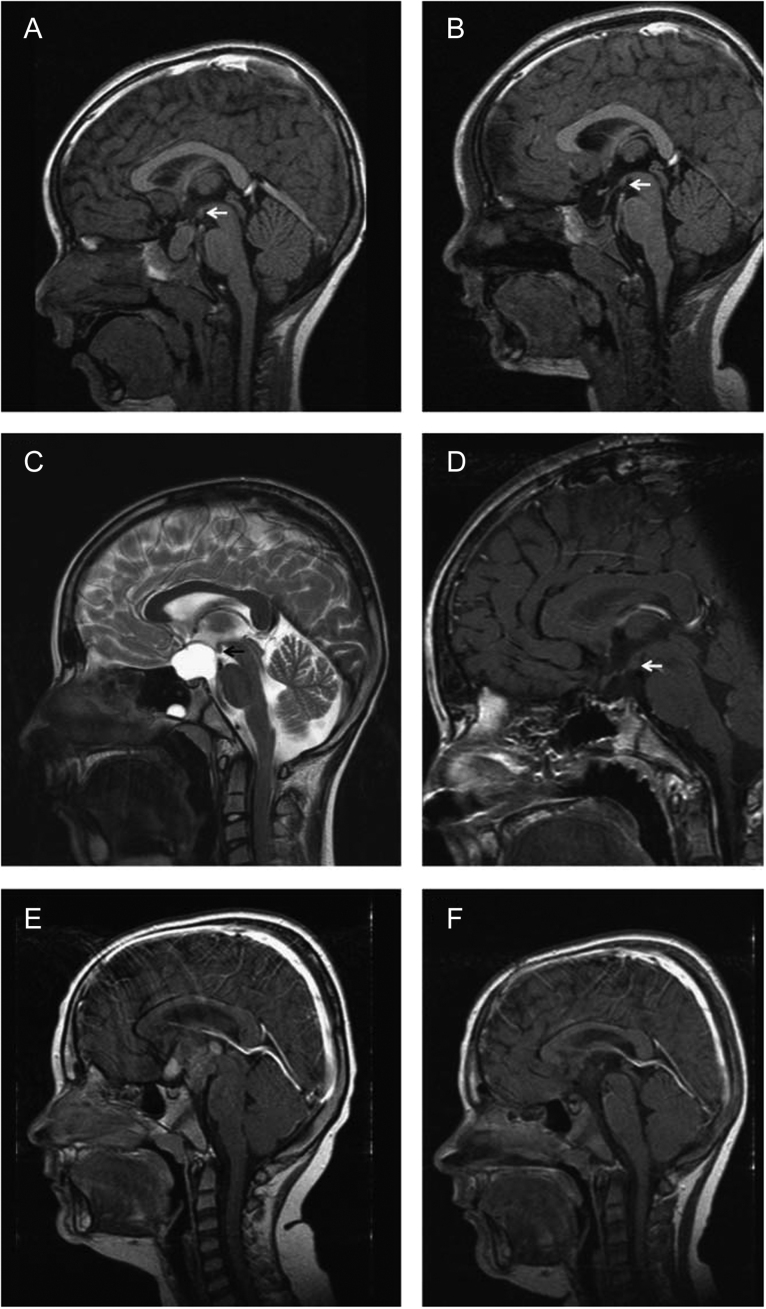
Figures
References
-
- van Iersel L, Brokke KE, Adan RAH, Bulthuis LCM, van den Akker ELT, van Santen HM. Pathophysiology and individualized treatment of hypothalamic obesity following craniopharyngioma and other suprasellar tumors: a systematic review. Endocrine Reviews 201940193–235. ( 10.1210/er.2018-00017) - DOI - PubMed
LinkOut - more resources
Full Text Sources
