

Modulation of BCL-2 in Both T Cells and Tumor Cells to Enhance Chimeric Antigen Receptor T-cell Immunotherapy against Cancer
- PMID: 35904479
- PMCID: PMC9547936
- DOI: 10.1158/2159-8290.CD-21-1026
Modulation of BCL-2 in Both T Cells and Tumor Cells to Enhance Chimeric Antigen Receptor T-cell Immunotherapy against Cancer
Abstract
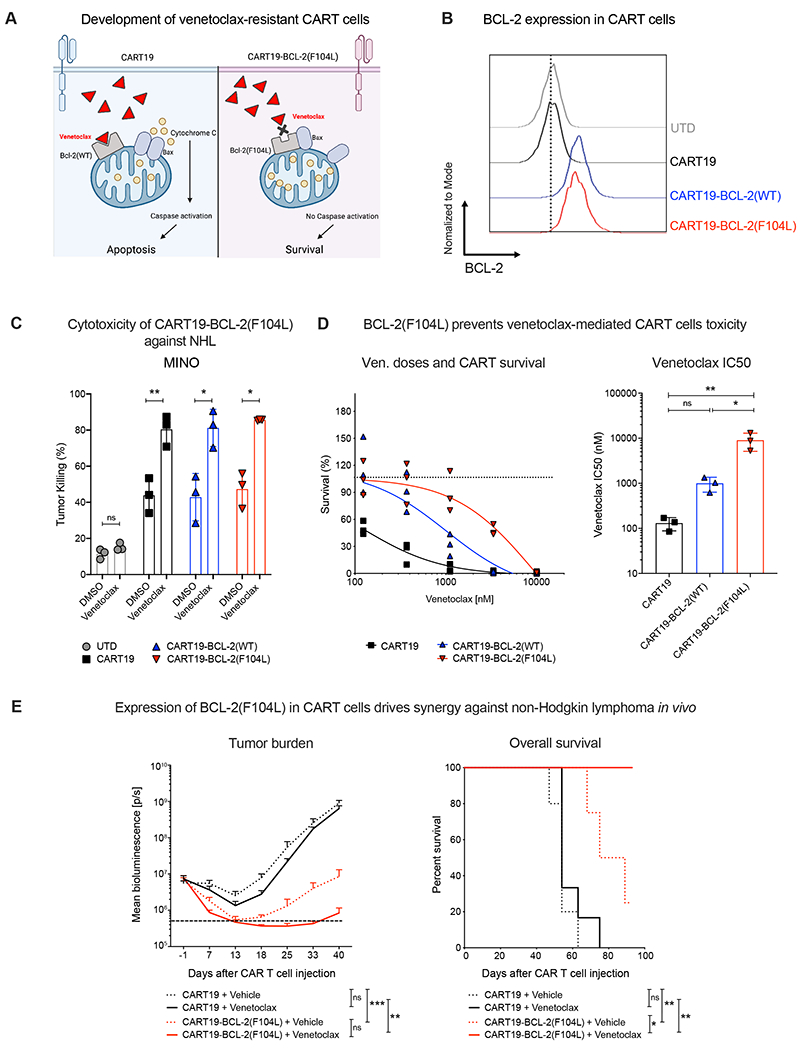
Chimeric antigen receptor T-cell (CART) immunotherapy led to unprecedented responses in patients with refractory/relapsed B-cell non-Hodgkin lymphoma (NHL); nevertheless, two thirds of patients experience treatment failure. Resistance to apoptosis is a key feature of cancer cells, and it is associated with treatment failure. In 87 patients with NHL treated with anti-CD19 CART, we found that chromosomal alteration of B-cell lymphoma 2 (BCL-2), a critical antiapoptotic regulator, in lymphoma cells was associated with reduced survival. Therefore, we combined CART19 with the FDA-approved BCL-2 inhibitor venetoclax and demonstrated in vivo synergy in venetoclax-sensitive NHL. However, higher venetoclax doses needed for venetoclax-resistant lymphomas resulted in CART toxicity. To overcome this limitation, we developed venetoclax-resistant CART by overexpressing mutated BCL-2(F104L), which is not recognized by venetoclax. Notably, BCL-2(F104L)-CART19 synergized with venetoclax in multiple lymphoma xenograft models. Furthermore, we uncovered that BCL-2 overexpression in T cells intrinsically enhanced CART antitumor activity in preclinical models and in patients by prolonging CART persistence.
Significance: This study highlights the role of BCL-2 in resistance to CART immunotherapy for cancer and introduces a novel concept for combination therapies-the engineering of CART cells to make them resistant to proapoptotic small molecules, thereby enhancing the therapeutic index of these combination therapies. This article is highlighted in the In This Issue feature, p. 2221.
©2022 American Association for Cancer Research.
Figures





References
-
- Chong EA, Ruella M, Schuster SJ. Five-year outcomes for refractory B-cell lymphomas with CAR T-cell therapy. New England Journal of Medicine 2021;384(7):673–4. - PubMed
-
- Ruella M, Gill S. How to train your T cell: genetically engineered chimeric antigen receptor T cells versus bispecific T-cell engagers to target CD19 in B acute lymphoblastic leukemia. Expert opinion on biological therapy 2015;15(6):761–6. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Molecular Biology Databases
