

Dissecting drivers of immune activation in chronic HIV-1 infection
- PMID: 35905559
- PMCID: PMC9334338
- DOI: 10.1016/j.ebiom.2022.104182
Dissecting drivers of immune activation in chronic HIV-1 infection
Abstract
Background: Immune activation is a significant contributor to HIV pathogenesis and disease progression. In virally-suppressed individuals on ART, low-level immune activation has been linked to several non-infectious comorbid diseases. However, studies have not been systematically performed in sub-Saharan Africa and thus the impact of demographics, ART and regional endemic co-infections on immune activation is not known. We therefore comprehensively evaluated in a large multinational African cohort markers for immune activation and its distribution in various settings.
Methods: 2747 specimens from 2240 people living with HIV (PLWH) and 477 without HIV from the observational African Cohort Study (AFRICOS) were analyzed for 13 immune parameters. Samples were collected along with medical history, sociodemographic and comorbidity data at 12 HIV clinics across 5 programs in Uganda, Kenya, Tanzania and Nigeria. Data were analyzed with univariate and multivariate methods such as random forests and principal component analysis.
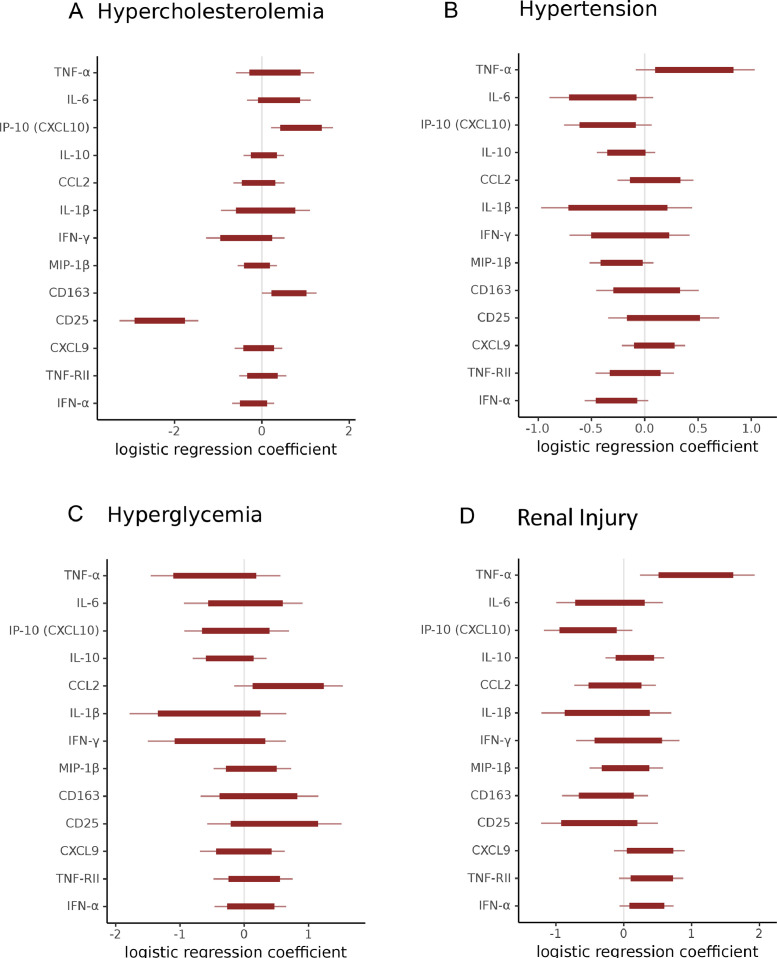
Findings: Immune activation was markedly different between PLWH with detectable viral loads, and individuals without HIV across sites. Among viremic PLWH, we found that all immune parameters were significantly correlated with viral load except for IFN-α. The overall inflammatory profile was distinct between men and women living with HIV, in individuals off ART and with HIV viremia. We observed stronger differences in the immune activation profile with increasing viremia. Using machine learning methods, we found that geographic differences contributed to unique inflammatory profiles. We also found that among PLWH, age and the presence of infectious and/or noninfectious comorbidities showed distinct inflammatory patterns, and biomarkers may be used to predict the presence of some comorbidities.
Interpretation: Our findings show that chronic immune activation in HIV-1 infection is influenced by HIV viral load, sex, age, region and ART use. These predictors, as well as associations among some biomarkers and coinfections, influence biomarkers associated with noncommunicable diseases.
Funding: This work was supported by the President's Emergency Plan for AIDS Relief via a cooperative agreement between the Henry M. Jackson Foundation for the Advancement of Military Medicine, Inc., and the U.S. Department of Defense [W81XWH-11-2-0174, W81XWH-18-2-0040]. The investigators have adhered to the policies for protection of human subjects as prescribed in AR 70-25. This article was prepared while Michael A. Eller was employed at Henry M. Jackson Foundation for the Advancement of Military Medicine for the U.S. Military HIV Research Program. The views expressed are those of the authors and should not be construed to represent the positions of the US Army or the Department of Defense. The opinions expressed in this article are the author's own, and do not reflect the view of the National Institutes of Health, the U.S. Department of Health and Human Services, or the U.S. government.
Keywords: Antiretroviral therapy; HIV; Immune activation; Inflammation.
Copyright © 2022 The Author(s). Published by Elsevier B.V. All rights reserved.
Conflict of interest statement
Declaration of interests All authors declare no conflicts of interest.
Figures




References
-
- Wing E.J. HIV and aging. Int J Infect Dis. 2016;53:61–68. - PubMed
-
- Guaraldi G., Milic J., Mussini C. Aging with HIV. Curr HIV/AIDS Rep. 2019;16(6):475–481. - PubMed
-
- Franceschi C., Bonafé M., Valensin S., et al. Inflamm-aging. An evolutionary perspective on immunosenescence. Ann N Y Acad Sci. 2000;908:244–254. - PubMed
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Research Materials
