

Assessing clinical utility of preconception expanded carrier screening regarding residual risk for neurodevelopmental disorders
- PMID: 35906228
- PMCID: PMC9338263
- DOI: 10.1038/s41525-022-00316-x
Assessing clinical utility of preconception expanded carrier screening regarding residual risk for neurodevelopmental disorders
Abstract
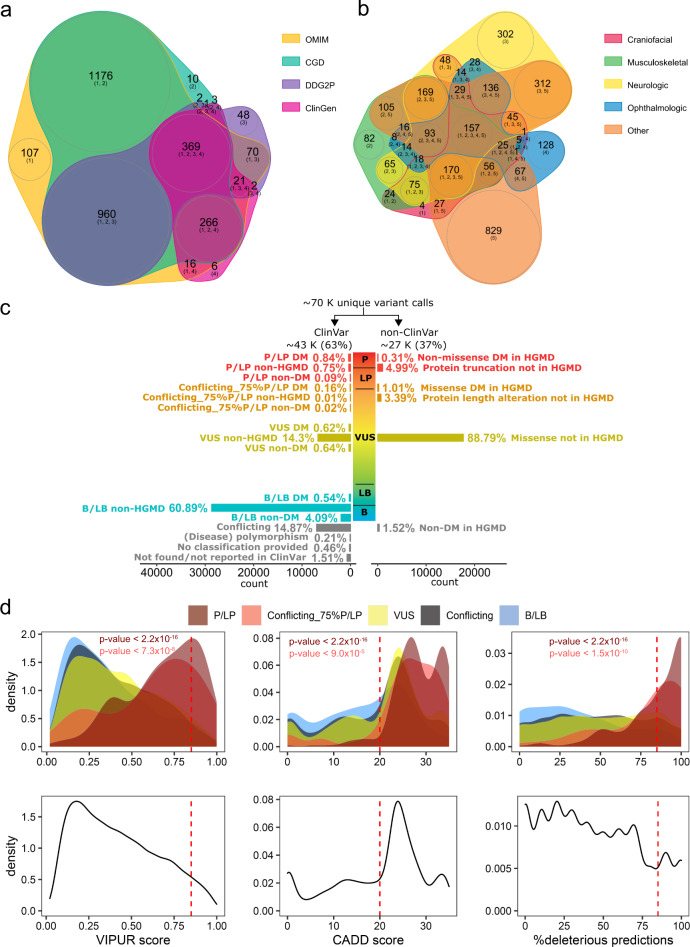
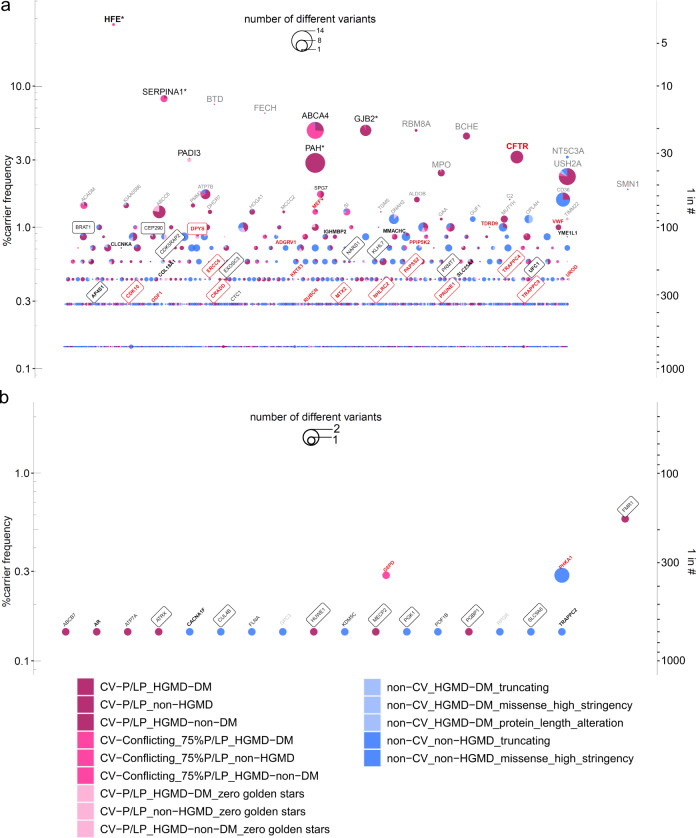
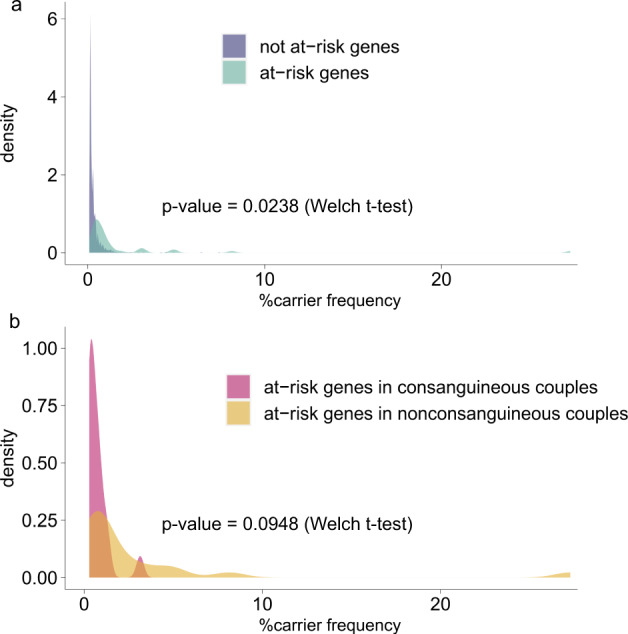
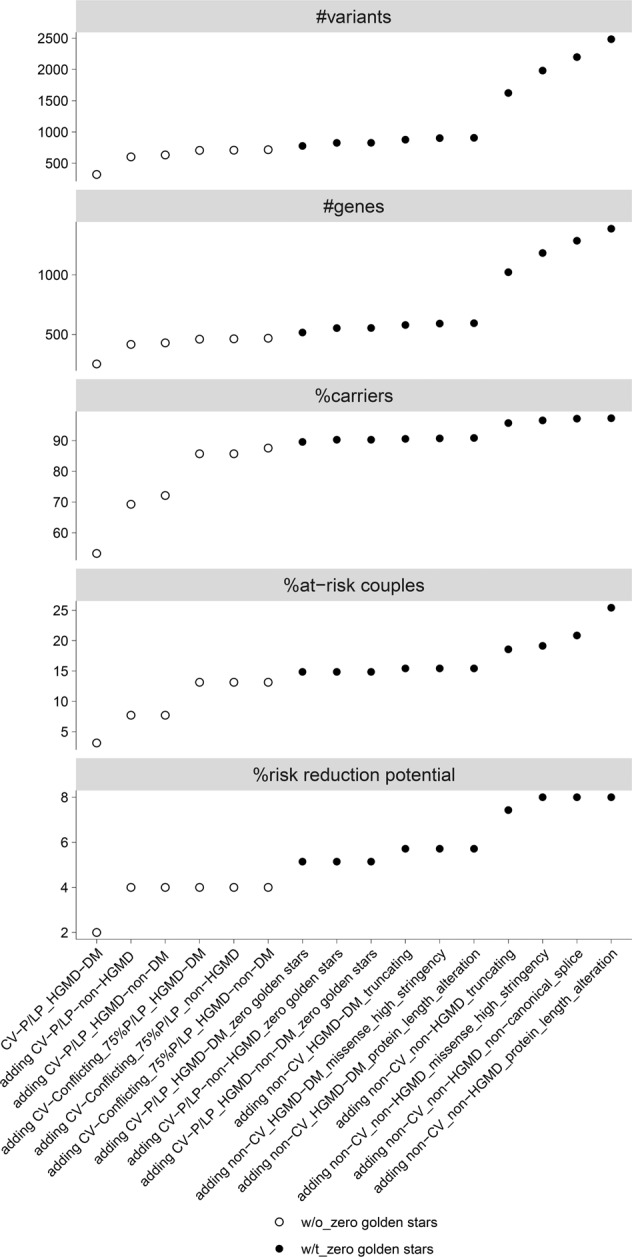
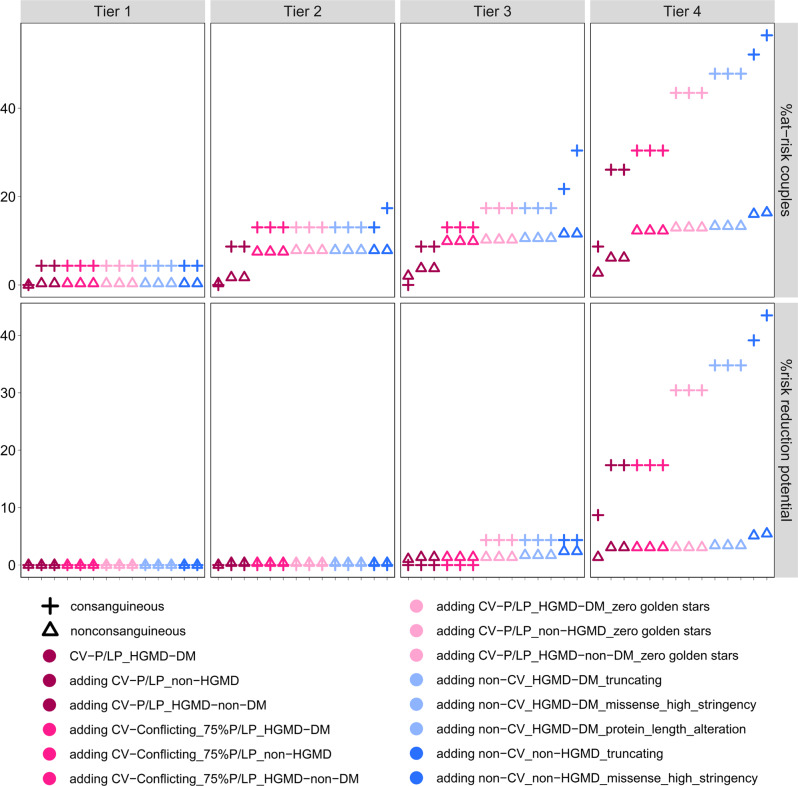
The magnitude of clinical utility of preconception expanded carrier screening (ECS) concerning its potential to reduce the risk of affected offspring is unknown. Since neurodevelopmental disorders (NDDs) in their offspring is a major concern of parents-to-be, we addressed the question of residual risk by assessing the risk-reduction potential for NDDs in a retrospective study investigating ECS with different criteria for gene selection and definition of pathogenicity. We used exome sequencing data from 700 parents of children with NDDs and blindly screened for carrier-alleles in up to 3046 recessive/X-linked genes. Depending on variant pathogenicity thresholds and gene content, NDD-risk-reduction potential was up to 43.5% in consanguineous, and 5.1% in nonconsanguineous couples. The risk-reduction-potential was compromised by underestimation of pathogenicity of missense variants (false-negative-rate 4.6%), inherited copy-number variants and compound heterozygosity of one inherited and one de novo variant (0.9% each). Adherence to the ACMG recommendations of restricting ECS to high-frequency genes in nonconsanguineous couples would more than halve the detectable inherited NDD-risk. Thus, for optimized clinical utility of ECS, screening in recessive/X-linked genes regardless of their frequency (ACMG Tier-4) and sensible pathogenicity thresholds should be considered for all couples seeking ECS.
© 2022. The Author(s).
Conflict of interest statement
The authors declare no competing interests.
Figures
Similar articles
-
Clinical validity and utility of preconception expanded carrier screening for the management of reproductive genetic risk in IVF and general population.Hum Reprod. 2021 Jun 18;36(7):2050-2061. doi: 10.1093/humrep/deab087. Hum Reprod. 2021. PMID: 34021342
-
Carrier frequency estimation of pathogenic variants of autosomal recessive and X-linked recessive mendelian disorders using exome sequencing data in 1,642 Thais.BMC Med Genomics. 2024 Jan 2;17(1):9. doi: 10.1186/s12920-023-01771-w. BMC Med Genomics. 2024. PMID: 38167091 Free PMC article.
-
Experience using singleton exome sequencing of probands as an approach to preconception carrier screening in consanguineous couples.J Med Genet. 2023 Jun;60(6):540-546. doi: 10.1136/jmg-2022-108607. Epub 2022 Dec 8. J Med Genet. 2023. PMID: 36600615
-
Interest in expanded carrier screening among individuals and couples in the general population: systematic review of the literature.Hum Reprod Update. 2020 Apr 15;26(3):335-355. doi: 10.1093/humupd/dmaa001. Hum Reprod Update. 2020. PMID: 32099997
-
Prenatal genetic carrier screening in the genomic age.Semin Perinatol. 2018 Aug;42(5):303-306. doi: 10.1053/j.semperi.2018.07.019. Epub 2018 Jul 26. Semin Perinatol. 2018. PMID: 30241949 Review.
Cited by
-
Regional patterns of genetic variants in expanded carrier screening: a next-generation sequencing pilot study in Fujian Province, China.Front Genet. 2025 May 12;16:1527228. doi: 10.3389/fgene.2025.1527228. eCollection 2025. Front Genet. 2025. PMID: 40421383 Free PMC article.
-
Estimating at-risk couple rates across 1000 exome sequencing data cohort for 176 genes and its importance relevance for health policies.Eur J Hum Genet. 2025 Jan;33(1):65-71. doi: 10.1038/s41431-024-01726-4. Epub 2024 Nov 2. Eur J Hum Genet. 2025. PMID: 39488673
-
Couple-Based Carrier Screening: How Gene and Variant Considerations Impact Outcomes.Genes (Basel). 2025 May 30;16(6):671. doi: 10.3390/genes16060671. Genes (Basel). 2025. PMID: 40565563 Free PMC article.
-
Pregnancy Planning and Genetic Testing: Exploring Advantages, and Challenges.Genes (Basel). 2024 Sep 13;15(9):1205. doi: 10.3390/genes15091205. Genes (Basel). 2024. PMID: 39336796 Free PMC article. Review.
References
-
- Kaback, M. M. Population-based genetic screening for reproductive counseling: The Tay-Sachs disease model. in European Journal of Pediatrics, Supplement159, (Springer Verlag, 2000). - PubMed
Grants and funding
LinkOut - more resources
Full Text Sources
