

Influence of diabetes on mortality and ICD therapies in ICD recipients: a systematic review and meta-analysis of 162,780 patients
- PMID: 35906611
- PMCID: PMC9338523
- DOI: 10.1186/s12933-022-01580-y
Influence of diabetes on mortality and ICD therapies in ICD recipients: a systematic review and meta-analysis of 162,780 patients
Abstract
Background: The influence of diabetes on the mortality and risk of implantable cardioverter defibrillator (ICD) therapies is still controversial, and a comprehensive assessment is lacking. We performed this systematic review and meta-analysis to address this controversy.
Methods: We systematically searched the PubMed, Embase, Web of Science and Cochrane Library databases to collect relevant literature. Fixed and random effects models were used to estimate the hazard ratio (HR) with 95% CIs.
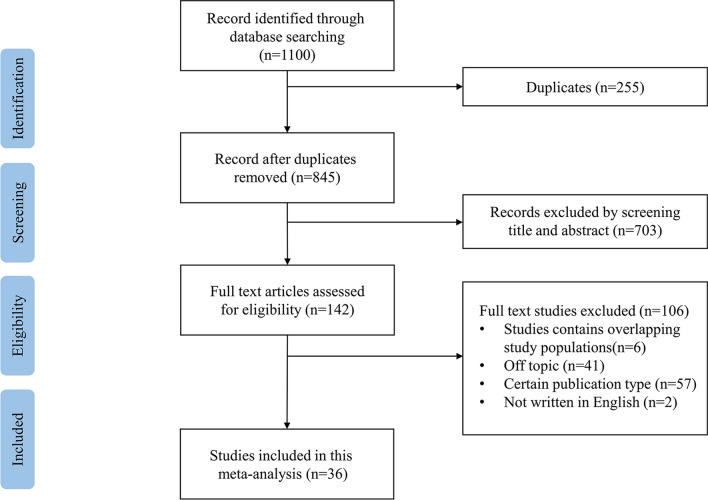
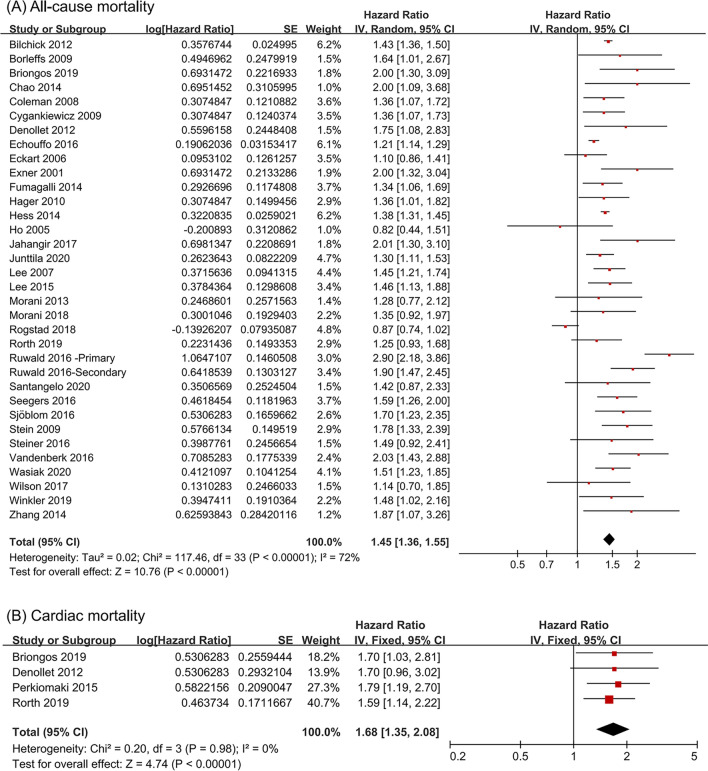
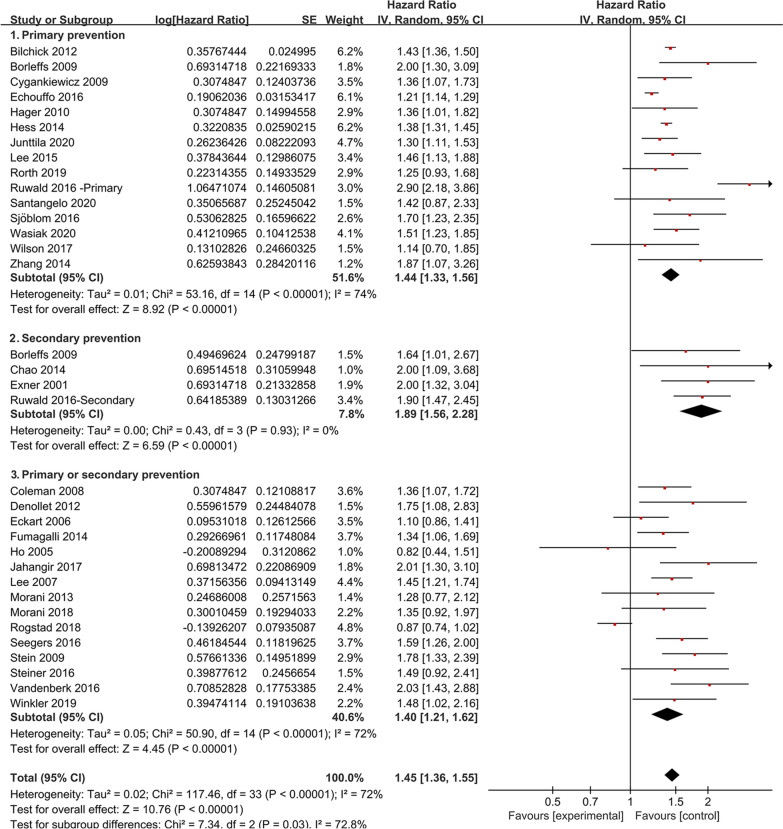
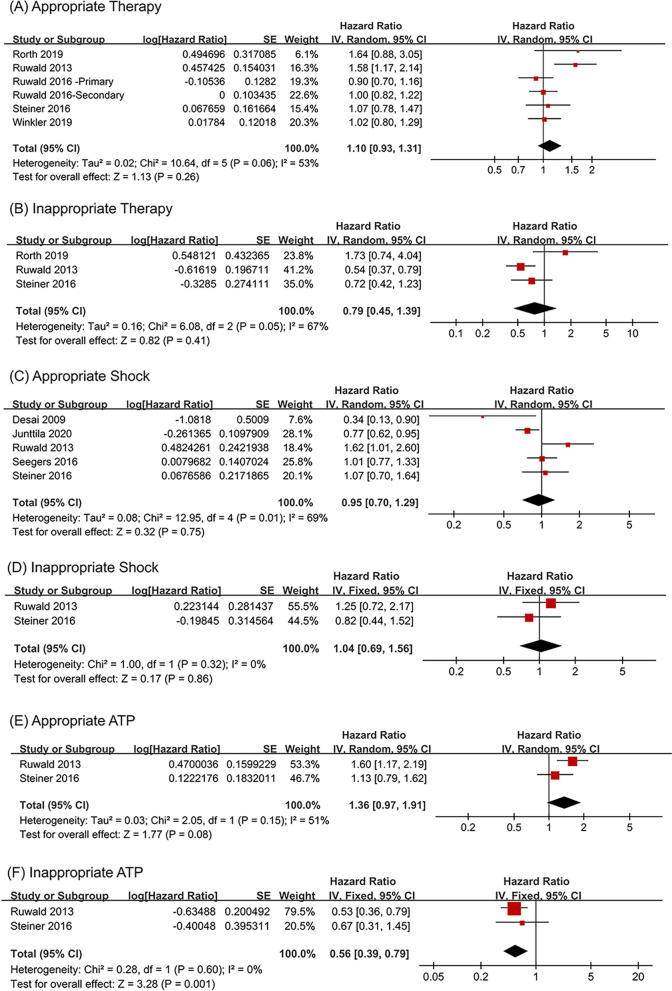
Results: Thirty-six articles reporting on 162,780 ICD recipients were included in this analysis. Compared with nondiabetic ICD recipients, diabetic ICD recipients had higher all-cause mortality (HR = 1.45, 95% CI 1.36-1.55). The subgroup analysis showed that secondary prevention patients with diabetes may suffer a higher risk of all-cause mortality (HR = 1.89, 95% CI 1.56-2.28) (for subgroup analysis, P = 0.03). Cardiac mortality was also higher in ICD recipients with diabetes (HR = 1.68, 95% CI 1.35-2.08). However, diabetes had no significant effect on the risks of ICD therapies, including appropriate or inappropriate therapy, appropriate or inappropriate shock and appropriate anti-tachycardia pacing (ATP). Diabetes was associated with a decreased risk of inappropriate ATP (HR = 0.56, 95% CI 0.39-0.79).
Conclusion: Diabetes is associated with an increased risk of mortality in ICD recipients, especially in the secondary prevention patients, but does not significantly influence the risks of ICD therapies, indicating that the increased mortality of ICD recipients with diabetes may not be caused by arrhythmias. The survival benefits of ICD treatment in diabetes patients are limited.
Keywords: Diabetes; ICD recipients; ICD therapies; Influence; Mortality.
© 2022. The Author(s).
Conflict of interest statement
The authors declare that they have no competing interests.
Figures
Similar articles
-
Meta-Analysis of Risk of Ventricular Arrhythmias and All-Cause Mortality in Patients With Chronic Total Occlusion of a Coronary Artery and/or Implantable Cardioverter-Defibrillator.Am J Cardiol. 2018 May 15;121(10):1149-1154. doi: 10.1016/j.amjcard.2018.02.001. Epub 2018 Feb 12. Am J Cardiol. 2018. PMID: 29548677
-
A Decision Tree-Based Survival Analysis of Patients with a History of Inappropriate Implantable Cardioverter-Defibrillator Therapy.Int Heart J. 2019 Mar 20;60(2):318-326. doi: 10.1536/ihj.18-288. Epub 2019 Feb 8. Int Heart J. 2019. PMID: 30745538
-
Mortality Implications of Appropriate Implantable Cardioverter Defibrillator Therapy in Secondary Prevention Patients: Contrasting Mortality in Primary Prevention Patients From a Prospective Population-Based Registry.J Am Heart Assoc. 2017 Aug 19;6(8):e006220. doi: 10.1161/JAHA.117.006220. J Am Heart Assoc. 2017. PMID: 28862957 Free PMC article.
-
Implantable cardioverter-defibrillators in cardiac transplant recipients: A systematic review from the Electrophysiology Collaborative Consortium for Meta-analysis-ELECTRAM investigators.Pacing Clin Electrophysiol. 2020 Dec;43(12):1529-1537. doi: 10.1111/pace.14098. Epub 2020 Nov 12. Pacing Clin Electrophysiol. 2020. PMID: 33180346
-
Systematic Review and Meta-Analysis of Clinical Outcome After Implantable Cardioverter-Defibrillator Therapy in Patients With Chagas Heart Disease.JACC Clin Electrophysiol. 2019 Oct;5(10):1213-1223. doi: 10.1016/j.jacep.2019.07.003. Epub 2019 Aug 28. JACC Clin Electrophysiol. 2019. PMID: 31648747
Cited by
-
Implantable Cardioverter Defibrillator Tachycardia Therapies: Past, Present and Future Directions.J Cardiovasc Dev Dis. 2024 Mar 20;11(3):92. doi: 10.3390/jcdd11030092. J Cardiovasc Dev Dis. 2024. PMID: 38535115 Free PMC article. Review.
-
Implantable Cardioverter-Defibrillators Among Older Survivors of Out-of-Hospital Cardiac Arrest.J Am Heart Assoc. 2024 Oct;13(19):e036123. doi: 10.1161/JAHA.124.036123. Epub 2024 Sep 18. J Am Heart Assoc. 2024. PMID: 39291485 Free PMC article.
References
-
- International Diabetes Federation . IDF diabetes atlas. 10. Brussels: International Diabetes Federation; 2021. - PubMed
-
- Sarwar N, Gao P, Seshasai SR, Gobin R, Kaptoge S, Di Angelantonio E, Ingelsson E, Lawlor DA, Selvin E, Emerging Risk Factors C et al. Diabetes mellitus, fasting blood glucose concentration, and risk of vascular disease: a collaborative meta-analysis of 102 prospective studies. Lancet. 2010;375(9733):2215–2222. doi: 10.1016/S0140-6736(10)60484-9. - DOI - PMC - PubMed
-
- MacDonald MR, Petrie MC, Varyani F, Ostergren J, Michelson EL, Young JB, Solomon SD, Granger CB, Swedberg K, Yusuf S, et al. Impact of diabetes on outcomes in patients with low and preserved ejection fraction heart failure: an analysis of the candesartan in heart failure: assessment of reduction in mortality and morbidity (CHARM) programme. Eur Heart J. 2008;29(11):1377–1385. doi: 10.1093/eurheartj/ehn153. - DOI - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
