

Intraoperative fluoroscopic protocol to avoid rotational malalignment after nailing of tibia shaft fractures: introduction of the 'C-Arm Rotational View (CARV)'
- PMID: 35907028
- PMCID: PMC10728226
- DOI: 10.1007/s00068-022-02038-2
Intraoperative fluoroscopic protocol to avoid rotational malalignment after nailing of tibia shaft fractures: introduction of the 'C-Arm Rotational View (CARV)'
Erratum in
-
Correction: Intraoperative fluoroscopic protocol to avoid rotational malalignment after nailing of tibia shaft fractures: introduction of the 'C-Arm Rotational View (CARV)'.Eur J Trauma Emerg Surg. 2023 Dec;49(6):2337. doi: 10.1007/s00068-022-02098-4. Eur J Trauma Emerg Surg. 2023. PMID: 36413268 Free PMC article. No abstract available.
Abstract
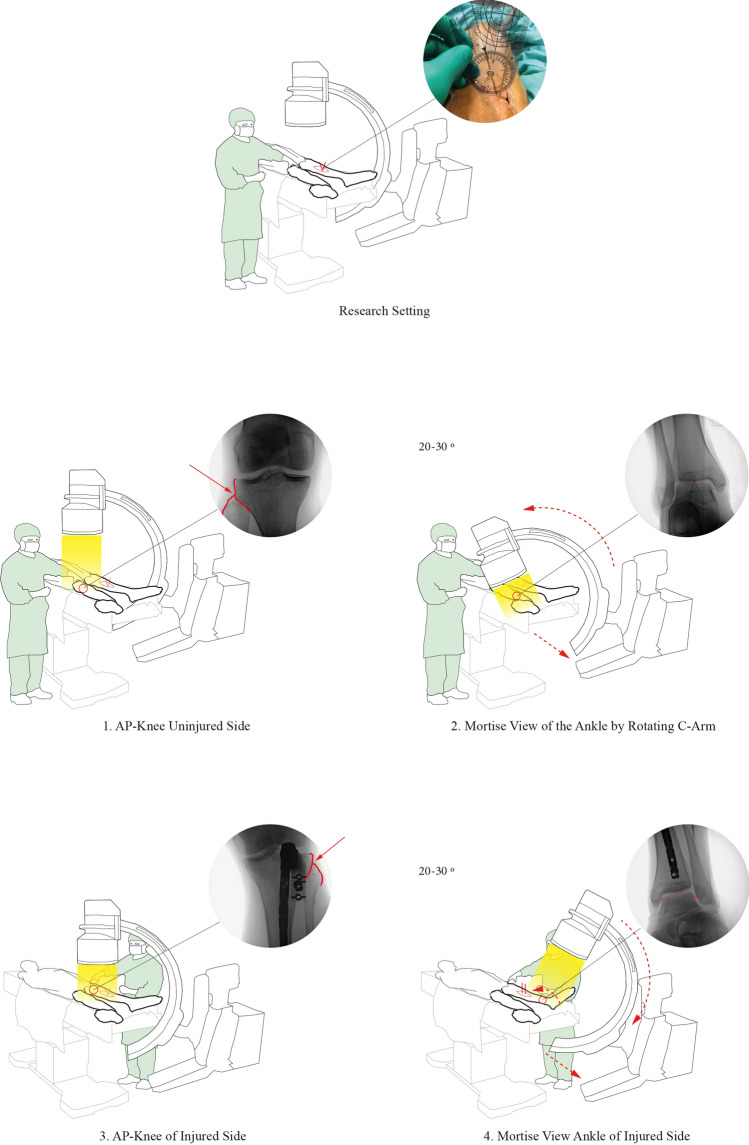
Purpose: Rotational malalignment (≥ 10°) is a frequent pitfall of intramedullary-nailing of tibial shaft fractures. This study aimed to develop an intraoperative fluoroscopy protocol, coined 'C-Arm Rotational View (CARV)', to significantly reduce the risk for rotational malalignment and to test its clinical feasibility.
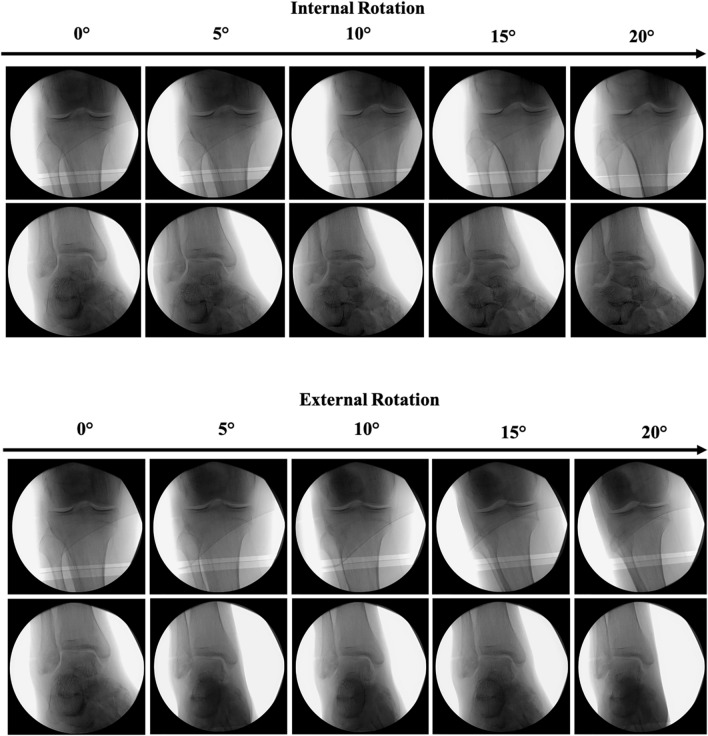
Methods: A cadaver and clinical feasibility study was conducted to develop the CARV-technique, that included a standardized intraoperative fluoroscopy sequence of predefined landmarks on the uninjured and injured leg in which the rotation of the C-arm was used to verify for rotational alignment. A mid-shaft tibia fracture was simulated in a cadaver and an unlocked intramedullary-nail was inserted. Random degrees of rotational malalignment were applied using a hand-held goniometer via reference wires at the fracture site. Ten surgeons, blinded for the applied rotation, performed rotational corrections according to (1) current clinical practice after single-leg and dual-leg draping, and (2) according to the CARV-protocol. The primary outcome measure was the accuracy of the corrections relative to neutral tibial alignment. The CARV-protocol was tested in a small clinical cohort.
Results: In total, 180 rotational corrections were performed by 10 surgeons. Correction according to clinical practice using single-leg and dual-leg draping resulted in a median difference of, respectively, 10.0° (IQR 5.0°) and 10.0° (IQR 5.0°) relative to neutral alignment. Single-leg and dual-leg draping resulted in malalignment (≥10°) in, respectively, 67% and 58% of the corrections. Standardized correction using the CARV resulted in a median difference of 5.0° (IQR 5.0°) relative to neutral alignment, with only 12% categorized as malalignment (≥10°). The incidence of rotational malalignment after application of the CARV decreased from 67% and 58% to 12% (p = <0.001). Both consultants and residents successfully applied the CARV-protocol. Finally, three clinical patients with a tibial shaft fracture were treated according to the CARV-protocol, resulting all in acceptable alignment (<10°) based on postoperative CT-measurements.
Conclusion: This study introduces an easy-to-use and clinically feasible standardized intraoperative fluoroscopy protocol coined 'C-arm rotational view (CARV)' to minimize the risk for rotational malalignment following intramedullary-nailing of tibial shaft fractures.
Keywords: Intramedullary-nailing; Rotational malalignment; Tibia shaft fractures; ‘C-Arm Rotational View (CARV)’.
© 2022. The Author(s).
Conflict of interest statement
None.
Figures
References
-
- Khan SB, Mohib Y, Rashid RH, Rashid H. Rotational mal-alignment after reamed intramedullary nailing for tibial shaft fracture. J Pak Med Assoc. 2016;66(3):S106–S108. - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
