

Vessel wall MR imaging in neuroradiology
- PMID: 35907157
- PMCID: PMC9362557
- DOI: 10.1007/s11547-022-01528-y
Vessel wall MR imaging in neuroradiology
Abstract
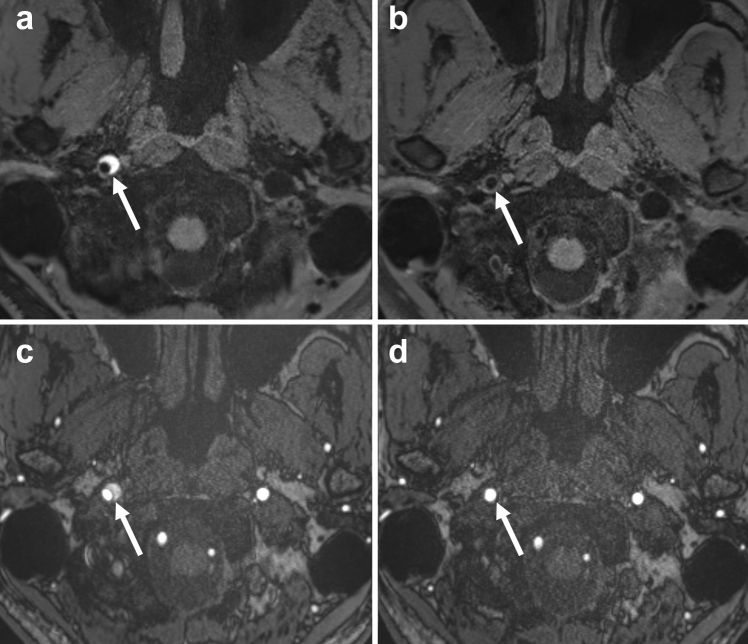
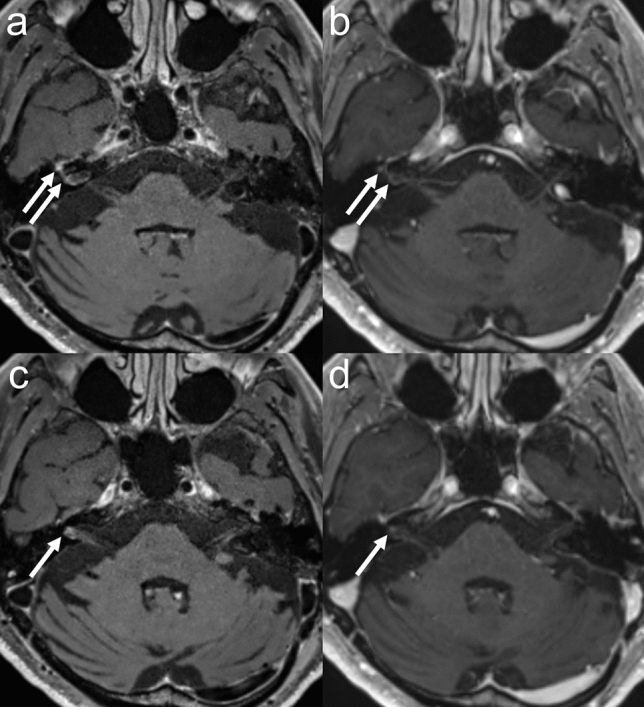
Vessel wall MR imaging (VW-MRI) has been introduced into clinical practice and applied to a variety of diseases, and its usefulness has been reported. High-resolution VW-MRI is essential in the diagnostic workup and provides more information than other routine MR imaging protocols. VW-MRI is useful in assessing lesion location, morphology, and severity. Additional information, such as vessel wall enhancement, which is useful in the differential diagnosis of atherosclerotic disease and vasculitis could be assessed by this special imaging technique. This review describes the VW-MRI technique and its clinical applications in arterial disease, venous disease, vasculitis, and leptomeningeal disease.
Keywords: 3D MRI; Delay alternating with nutation for tailored excitation; MR angiography; Magnetization transfer; Vessel wall MR imaging; Vessel wall enhancement.
© 2022. Italian Society of Medical Radiology.
Conflict of interest statement
The authors have no relevant financial or non-financial interest to disclose.
Figures






References
-
- Adams HP, Jr, Bendixen BH, Kappelle LJ, Biller J, Love BB, Gordon DL, Marsh EE., 3rd Classification of subtype of acute ischemic stroke. Definitions for use in a multicenter clinical trial. TOAST. Trial of org 10172 in acute stroke treatment. Stroke. 1993;24(1):35–41. doi: 10.1161/01.str.24.1.35. - DOI - PubMed
-
- Ay H, Arsava EM, Andsberg G, Benner T, Brown RD, Jr, Chapman SN, Cole JW, Delavaran H, Dichgans M, Engstrom G, Giralt-Steinhauer E, Grewal RP, Gwinn K, Jern C, Jimenez-Conde J, Jood K, Katsnelson M, Kissela B, Kittner SJ, Kleindorfer DO, Labovitz DL, Lanfranconi S, Lee JM, Lehm M, Lemmens R, Levi C, Li L, Lindgren A, Markus HS, McArdle PF, Melander O, Norrving B, Peddareddygari LR, Pedersen A, Pera J, Rannikmae K, Rexrode KM, Rhodes D, Rich SS, Roquer J, Rosand J, Rothwell PM, Rundek T, Sacco RL, Schmidt R, Schurks M, Seiler S, Sharma P, Slowik A, Sudlow C, Thijs V, Woodfield R, Worrall BB, Meschia JF. Pathogenic ischemic stroke phenotypes in the NINDS-stroke genetics network. Stroke. 2014;45(12):3589–3596. doi: 10.1161/STROKEAHA.114.007362. - DOI - PMC - PubMed
-
- Cappendijk VC, Cleutjens KB, Kessels AG, Heeneman S, Schurink GW, Welten RJ, Mess WH, Daemen MJ, van Engelshoven JM, Kooi ME. Assessment of human atherosclerotic carotid plaque components with multisequence MR imaging: initial experience. Radiology. 2005;234(2):487–492. doi: 10.1148/radiol.2342032101. - DOI - PubMed
